1 School of Graduate Studies, Rutgers University, Piscataway, New Jersey, USA
2 Department of Neuroscience and Cell Biology, Anatomical Association, Robert Wood Johnson Medical School, Rutgers University, Piscataway, New Jersey, USA
3 Department of Neuroscience and Cell Biology, Office of Education, Robert Wood Johnson Medical School, Rutgers University, Piscataway, New Jersey, USA
Durable anatomical teaching specimens are essential for extending learning beyond the dissection laboratory, particularly for anatomically complex structures that learners find difficult to conceptualize. While epoxy resin embedding has been described previously, most published protocols present finalized methods optimized for display, archival preservation, or research applications, with limited attention to pedagogical usability or protocol development. This study employed an iterative, trial-based methodological approach to develop an epoxy-resin protocol tailored for anatomy education. Using the brachial plexus as a test structure, three sequential embedding trials were conducted. Each trial introduced targeted methodological modifications informed by limitations identified in the preceding iteration. Variables systematically refined included resin selection, suspension strategies, pour volumes, de-bubbling techniques, and label integration. Specimens were evaluated following each trial for optical clarity, anatomical orientation, structural integrity, and suitability for instructional use. Progressive refinements across trials resulted in marked improvements in specimen clarity, stability, and preservation of three-dimensional anatomical relationships. Transitioning to a lower-exothermic epoxy formulation, implementing incremental low-volume pours, adopting a monofilament suspension system, and enhancing de-bubbling procedures collectively reduced tissue distortion and air entrapment. The final specimen demonstrated improved anatomical fidelity and incorporated embedded labels aligned with curricular learning objectives, enhancing pedagogical usability. This study presents a transparent, reproducible framework for developing epoxy-embedded anatomical teaching specimens through intentional, iterative refinement. Rather than proposing a universal protocol, the approach emphasizes methodological decision-making guided by educational priorities and realistic institutional constraints. The resulting protocol offers a low-cost, accessible option for creating high-fidelity teaching specimens that support active learning and extend anatomy education beyond the dissection laboratory.
epoxy resin embedding; plastination alternatives; resin embedding methodology; teaching specimens
Gail Elliott, Robert Wood Johnson Medical School, Rutgers University, New Jersey, USA
e-mail: ge111@rwjms.rutgers.edu

![]()



While resin embedding has been previously described as a method for preserving anatomical specimens, most existing reports present finalized or “universal” protocols optimized for display, archival preservation, or research applications (von Hagens et al., 1987; Latorre et al., 2007; Ravi & Bhat, 2011; Sora & Matusz, 2011; Pirici et al., 2023). In contrast, the present study adopts an iterative, trial-based methodological approach to systematically identify and address practical challenges involved in producing epoxy-embedded specimens specifically for anatomy education. Focusing on the brachial plexus, a spatially complex neuroanatomical structure that learners consistently find difficult, this work documents successive refinements in resin selection, suspension strategies, pour volumes, and de-bubbling techniques, with explicit attention to anatomical fidelity, orientation, and pedagogical usability. By foregrounding protocol optimization rather than end-state validation and situating methodological decisions within an educational context, this study provides a transparent and reproducible framework for institutions seeking low-cost, high-fidelity teaching specimens that extend learning beyond the dissection laboratory.
Mastery of human gross anatomy remains a cornerstone of medical and biomedical education, yet it presents persistent challenges for learners across undergraduate, graduate, and professional programs. Anatomy requires the rapid acquisition, retention, and application of large volumes of spatially complex information under significant time constraints. Although modern digital platforms offer interactive learning opportunities beyond traditional atlases, both digital and static resources may oversimplify anatomy and obscure the natural variation characteristic of real human structures (Lazarus et al., 2012; Netter, 2022; Drake et al., 2023). These limitations become particularly evident when access to human donor material is limited or temporally constrained, requiring learners to mentally reconstruct three-dimensional relationships without tangible reference materials (Mclachlan et al., 2004; Winkleman, 2007; Estai & Blunt, 2016). Human donor dissection remains widely regarded as the gold standard for anatomical education, offering unparalleled opportunities to observe authentic variation and integrate structural knowledge with clinical context (Winkleman, 2007; Lazarus et al., 2012; Estai & Blunt, 2016). However, institutional access to donor programs varies substantially, and even within well-resourced curricula, student exposure to human donor material is often brief. Consequently, there is a growing need for durable, portable anatomical teaching tools that extend learning beyond the dissection laboratory, particularly for anatomically complex regions such as neurovascular plexuses, where spatial relationships are difficult to conceptualize using two-dimensional resources alone (Turney, 2007; Sugand et al., 2010).
In parallel, contemporary medical and graduate-level education increasingly emphasizes active, student-centered learning strategies, including team-based learning (TBL), problem-based learning (PBL), and flipped classroom models. Accreditation standards now recommend that a substantial proportion of instructional time involves active learning approaches (Johnson, 2009; Burgess et al., 2020; LCME, 2024). Within anatomy education, TBL has been shown to enhance engagement, peer-to-peer learning, and assessment performance (Vasan et al., 2011; Parmlee et al., 2012; Burgess et al., 2017; Reimschisel et al., 2017). Nevertheless, students frequently report that active learning sessions may feel superficial when instructional materials lack sufficient realism or tactile engagement, particularly when learning relies primarily on digital images or schematic representations (Burgess et al., 2017). These observations highlight the importance of teaching tools that enhance the authenticity and pedagogical value of in-person learning environments. Historically, hands-on anatomical resources such as plastinated specimens, skeletal collections, and cross-sectional models have addressed this need by providing durable, high-fidelity representations of human anatomy (Azer & Eizenberg, 2007; McMenamin, 2008; Hashida et al., 2021). Plastination transformed anatomical preservation by producing long-lasting, odorless specimens with excellent structural stability (von Hagens et al., 1987; Latorre et al., 2007). Despite these advantages, plastination requires specialized facilities, extended processing times, and substantial financial investment, limiting its feasibility as an in-house solution for many institutions (Ravi & Bhat, 2011). The associated technical demands and chemical hazards present further barriers to widespread adoption.
As a result, alternative specimen preservation strategies, including silicone casting, polymer embedding, and three-dimensional printing, have been explored with varying success (von Hagens et al., 1987; Latorre et al., 2007; Ravi & Bhat, 2011; Pirici et al., 2023; Cadet Tomas et al., 2025). Among these, epoxy resin embedding offers a compelling balance of durability, transparency, and accessibility, as it can be implemented using commercially available materials and modest infrastructure (Thiel, 1992; Pirici et al., 2025). Nonetheless, epoxy embedding presents distinct technical challenges: exothermic curing reactions may damage delicate tissues, air entrapment can reduce visual clarity, and inadequate suspension techniques can compromise anatomical orientation (Holliday et al., 2001). These challenges are especially consequential when embedding intricate neuroanatomical structures intended for instructional use. Although prior studies have described epoxy or resin embedding protocols, most emphasize finalized methods optimized for display or research. Far less attention has been given to the iterative processes through which such protocols are developed and adapted to meet specific educational goals, leaving limited guidance for educators working within realistic institutional constraints.
Accordingly, this study reports an iterative, trial-based approach to developing epoxy-resin embedded human anatomical specimens designed explicitly to support anatomy education outside the dissection laboratory. Using the brachial plexus as a test case, three sequential embedding trials evaluated resin properties, mold design, suspension strategies, and bubble-reduction techniques. By documenting both procedural challenges and successive refinements, this work aims to provide a transparent and reproducible framework for educators seeking to create low-cost, high-fidelity anatomical teaching specimens aligned with active learning environments and curricular objectives. This study was designed as a structured methodological investigation, rather than a single finalized technique, in which successive embedding trials were compared and refined to generate an optimized, reproducible protocol for anatomy education. The hypothesis for this study was that progressive modifications in resin formulation, pour volume, suspension strategy, and de-bubbling will result in measurable improvements in specimen transparency and reduction of air entrapment.
Study Design and Methodological Rationale
This study employed an iterative, trial-based methodological design to develop and refine an epoxy resin embedding protocol designed for anatomy education. Rather than evaluating a single finalized procedure, three sequential embedding trials were conducted, with each trial informed by limitations identified in the preceding iteration. Methodological modifications were introduced systematically to address challenges related to optical clarity, anatomical orientation, exothermic tissue distortion, and pedagogical usability under realistic institutional constraints.
Specimen Acquisition and Preparation
Anatomical specimens were obtained from human donors previously preserved for educational purposes. All procedures adhered to ethical approval and institutional guidelines governing the use of donated human material through the Anatomical Association, Rutgers University. To accommodate mold dimensions while preserving anatomical continuity, the spinal cord was sectioned approximately 1 inch superior to the C5 nerve root and 3-4 inches inferior to the T1 nerve root. Peripheral nerve segments were selectively shortened as needed to fit within the mold while maintaining overall anatomical orientation and relational integrity.
During specimen preparation, emphasis was placed on preserving the major organizational elements of the brachial plexus (roots, trunks, divisions, cords, and terminal branches). However, there was no anatomical reason that smaller caliber branches were selectively trimmed. Instead, their omission was a deliberate, pragmatic decision aligned with the primary goal of the study, which was to develop a durable, clear, and instructionally practical teaching specimen rather than to produce a fully exhaustive anatomical preparation.
Preservation Protocol
Specimens were embalmed using an in-house preservation solution composed of phenol (15%), isopropyl alcohol (42.5%), and ethylene glycol (42.5%), supplemented with borax, potassium nitrate, and water. This formulation, consistent with previously reported protocols for plastination and resin embedding, provides both fixation and partial dehydration, thereby eliminating the need for additional drying steps (Henry & Nel, 1993). Over-dehydration was intentionally avoided to minimize tissue shrinkage and distortion that could compromise anatomical fidelity. Following dissection, specimens were removed using bone saws and bone cutters and temporarily stored in a 25% ethylene glycol solution, the in-house preservation method for neural tissues, to prevent desiccation or fungal growth until epoxy embedding was performed.
Evaluation Criteria
Specimen evaluation following each trial was conducted using structured observational criteria aligned with the instructional intention of the project. Although formal quantitative instrumentation was not employed, each outcome category was operationally defined to promote consistency across the trials. Optical clarity was assessed based on the visibility of deep anatomical structures through the resin block, the presence or absence of color distortion, and the degree of air bubble entrapment observable under standardized lighting conditions. Anatomical positioning was evaluated by comparing the orientation of roots, trunks, cords, and terminal branches to established anatomical references to determine whether three-dimensional relationships were preserved. Structural integrity was assessed by manual handling of the cured specimen, including resistance to deformation, absence of cracks or warping, and stability of embedded tissues during routine instructional manipulation. Suitability for educational use was determined by consultation with colleagues and alignment with curricular learning objectives. These assessments were intentionally pragmatic and education-focused, reflecting the exploratory aim of developing a functional teaching tool. The phrase “suitability for educational use” refers specifically to faculty-based assessment of whether the specimen would be practical and effective as a teaching aid. This determination was based on expert judgment rather than direct student testing or measurement of learning outcomes.
Overview of Embedding Trials
Three sequential embedding trials were conducted using brachial plexus specimens. Trial One established a baseline protocol using commercially available materials and basic suspension techniques. Trial Two introduced targeted methodological modifications to address limitations related to clarity, bubble formation, and anatomical distortion identified in Trial One. Trial Three further refined these procedures to optimize specimen stability, transparency, and instructional usability.
Trial One: Baseline Embedding Protocol
The initial embedding trial utilized CraftSmart™ “Clear Casting and Coating” epoxy resin. A semi-flexible silicone mold (volume 1,360 ml; 19 x 13 x 5 cm) was selected. Equal volumes of epoxy resin (component A) and epoxy hardener (component B) were mixed slowly and poured incrementally, with each layer measuring approximately 170 ml (~0.64 cm in depth). The initial pour served as a base layer and was allowed to partially cure for approximately 10 minutes prior to specimen placement. To maintain separation between the anterior and posterior cords of the brachial plexus, a rudimentary suspension system was constructed using forceps and office supplies (Fig. 1a).

Figure 1: Suspension strategies used to maintain anatomical orientation of the brachial plexus across sequential embedding trials. 1a: Trial One employed a rudimentary suspension system using forceps and office materials, which provided limited stabilization of the anterior and posterior cords. 1b: Trial Two introduced a monofilament fishing-line suspension system secured to an overhead frame, resulting in improved maintenance of three-dimensional anatomical relationships. Progressive refinement of suspension methods was central to reducing distortion and preserving instructional fidelity across trials.
Resin was mixed manually for 3 minutes and poured at 30-minute intervals until the mold was filled. The block was allowed to cure at room temperature for 48 hours before removal and evaluation. Following curing, the specimen was assessed for optical clarity, structural integrity, durability, and preservation of anatomical orientation (Fig. 2a). Limitations identified during Trial One, including suboptimal clarity, bubble formation, and challenges in maintaining stable anatomical positioning, informed subsequent methodological refinements.
Trial Two: Targeted Methodological Modifications
Trial Two was designed to address the limitations observed in Trial One. A rigid plastic mold with increased volume (2,700 ml; 29 x 18.5 x 5 cm) was used, and Superclear Tabletop Epoxy (Fiberglass Coatings™, FGCI) was selected to improve optical clarity and reduce bubble formation based on manufacturer specifications and prior reports. Pour volumes were increased to 337 ml per layer. Epoxy components were mixed using a dual-head electric mixer (Resiners™) for 4 minutes, followed by degassing for 12 minutes in a vacuum chamber (Aliestfdno™).
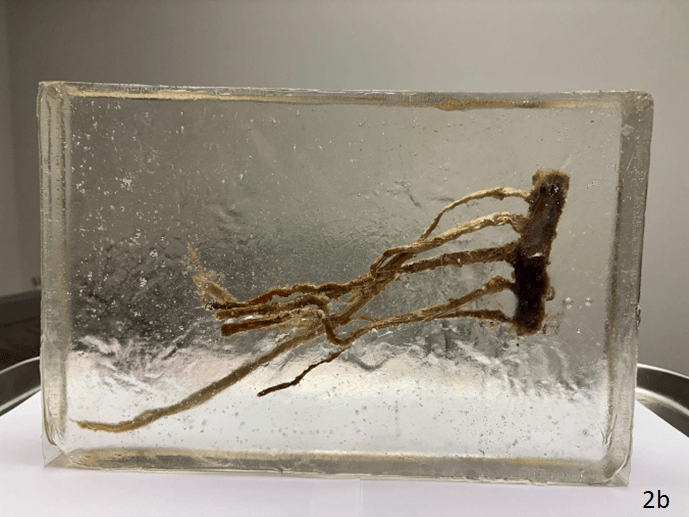
The initial resin layer was allowed to partially cure before specimen placement. Anatomical orientation was stabilized using a suspension system constructed from 2 Kg test monofilament fishing line threaded through thicker nerve segments and secured to an overhead wooden frame (Fig. 1b). This approach was intended to preserve the three-dimensional configuration of the brachial plexus. Layers were added sequentially at 30-minute intervals, with surface bubbles removed manually using a scalpel between pours. After the mold was filled, the specimen was cured at room temperature for 48 hours before removal and evaluation (Fig, 2b). Observations from Trial Two, particularly residual bubble formation and localized tissue distortion, guided further refinements introduced in Trial Three.
 |
 |
|
Figure 2: Final cured epoxy-embedded specimens produced during Trial One (2a) and Trial Two (2b). Trial One, utilizing CraftSmart™ epoxy and manual mixing, resulted in reduced optical clarity, yellow coloration immediately, and visible air entrapment. Visible damage is also seen to the specimen from the exothermic reaction between the epoxy resin and the hardener. Trial Two, incorporating FGCI epoxy, mechanical mixing, and vacuum degassing, demonstrated improved transparency and structural definition but retained localized distortion, severe bubble trapping, and the nerves were distorted and significantly shrunk away from the edges of the mold that they were 1.25 cm from. These observations informed further refinements introduced in Trial Three. |
|
Trial Three: Final Refinements for Instructional Use
Trial Three incorporated additional methodological refinements to further optimize clarity and minimize exothermic tissue distortion. The same rigid mold (2,700 ml) and FGCI epoxy resin were used. To reduce heat buildup during curing, resin was poured in smaller 50 ml increments (25 g epoxy resin, 25 g epoxy hardener; <0.6 cm depth). Prior to embedding, the specimen was pre-coated with two thin layers of resin applied using a fine paintbrush. This step was intended to stabilize anatomical orientation and buffer neural tissue from thermal effects during subsequent pours. Resin mixtures were degassed for 15 minutes using an alternative degassing device (Resiners™ Resin Bubble Remover), with additional 5-minute cycles performed as needed. After each pour, surface bubbles were removed using a heat gun (Calpalmy™). A light pad (Toheto™ A4 rechargeable Light Pad) was positioned beneath the mold to facilitate detection and removal of microbubbles.
To enhance instructional utility, clear adhesive labels identifying key components of the brachial plexus (roots, trunks, cords, and terminal branches) were produced using a P-Touch™ PTD 220 printer. Labels were waterproofed with sealant spray, pre-coated with resin, and embedded during intermediate layering stages to ensure stable placement. Following final curing at room temperature for 48 hours, the specimen was removed and evaluated (Fig. 3).
 |
 |
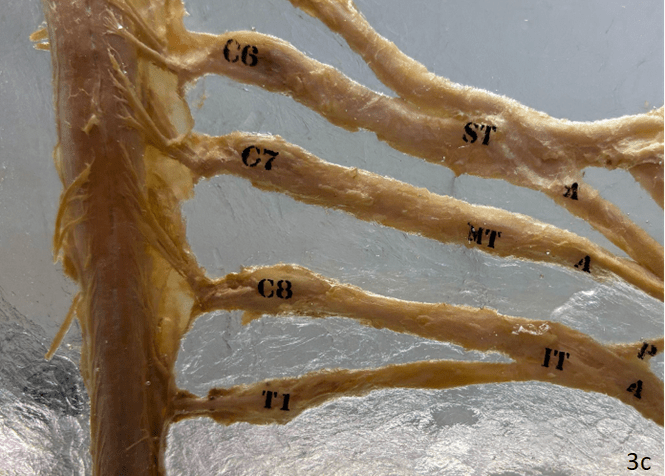 |
| Figure 3: Final epoxy-embedded brachial plexus specimen produced following Trial Three. Incremental low-volume pours, specimen pre-coating, enhanced de-bubbling procedures, and integrated labeling yielded improved optical clarity, reduced exothermic distortion, and stable anatomical orientation. Embedded labels identifying roots, trunks, cords, and terminal branches enhance pedagogical usability for anatomy instruction outside the dissection laboratory. | ||
Evaluation Criteria
Following each trial, specimens were evaluated by faculty reviewers for instructional practicality and handling suitability, rather than through formal classroom implementation. Assessment focused on the clarity of visible structures, stability during repeated handling, ease of demonstration in small-group settings, and alignment with intended curricular learning objectives. Students were not involved in the evaluation process, and no formal educational intervention was conducted as part of this study. Procedural challenges and improvements were documented across trials to inform subsequent refinements. A comparative summary of trial-specific advantages and limitations is presented in Table 1
| Features | Trial One | Trial Two | Trial Three |
| Mold volume | 1360 ml | 2700 ml | 2700 ml |
| Mold dimensions (cm) | 13 (w) x 19 (l) x 5 (h)
|
18.5 (w) x 29 (l) x 5 (h)
|
18.5 (w) x 29 (l) x 5 (h)
|
| Epoxy resin | CraftSmart™ “Clear Casting and Coating” | “Superclear Tabletop Epoxy” from Fiberglass Coatings™ (FGCI)” | “Superclear Tabletop Epoxy” from Fiberglass Coatings™ (FGCI)” |
| Pours/Layers | 170 ml (~0.6 cm per pour) | 337 ml (~1.2 cm per pour) | 50 ml (< 0.6 cm per pour) |
| De-bubble | Not implemented. | Aliestfdno Vacuum Degassing Chamber (12 minutes/ 2 cycles) |
Resiners resin bubble remove (10 minutes) CALPALMY™ bubble removing heat gun |
| Mixing | By hand (3 minutes) | Resiners™ Dual-Head Resin Mixer with Spiral Silicone Paddles (4 minutes/ 1 cycle) | ISTOYO™ Rechargeable Resin Mixer Ultra (4 minutes/ 1 cycle) |
| Positives | Fewer issues with bubble production during the mixing phases. | Clear coloration, quick drying times, very small exothermic reaction between epoxy and hardener. | Clear coloration, quick drying times, very small exothermic reaction between epoxy and hardener. |
| Negatives | Yellow coloration; strong exothermic reaction between the epoxy and hardener that seems to burn the neural tissues; lengthy drying times, final distortion of anatomy structures. | Production of small bubbles was a major issue that involved the incorporation of the de-bubbler into the process, which was not completely successful. More distortion of the anatomy structures in the final product. | Production of small bubbles was a major issue that involved the incorporation of the de-bubbler into the process, which was successful once the new de-bubbler and bubble removing gun were introduced. |
Final Protocol
Based on observations and refinements across the three sequential embedding trials, a final epoxy-resin embedding protocol was developed to optimize anatomical fidelity, optical clarity, and pedagogical usability for anatomy education. This protocol reflects methodological decisions informed by challenges identified during earlier trials, including exothermic tissue distortion, air entrapment, and instability of anatomical orientation. The steps outlined below represent the optimized procedure as implemented in Trial Three and are intended to be reproducible using commercially available materials and modest institutional infrastructure.
| Step | Instructions | Recommended Instruments/Materials |
| 1. | Specimen preparation and trimming:
Dissect and trim the brachial plexus specimen to fit the selected mold while preserving anatomical continuity and orientation. Section the spinal cord approximately 2.5 cm superior to the C5 nerve roots and 7.5–10 cm inferior to the T1 nerve roots. |
Scalpel, forceps |
| 2. | Short-term specimen storage:
Place the dissected specimen in a 25% ethylene glycol solution to prevent desiccation and microbial growth prior to embedding. |
25% ethylene glycol solution, sealable container |
| 3. | Mold selection and preparation:
Select a rigid mold with a capacity of approximately 2,700 mL (e.g., 18.5 x 29 x 5 cm). Ensure the mold is clean, dry, and level. Apply mold release spray to facilitate demolding. |
Rigid mold, level, lint-free wipes; Selsil mold release spray |
| 4. | Suspension system setup:
Construct and test a suspension system using a clear monofilament fishing line (2 kg test) secured to a stable overhead frame. This system should allow controlled positioning of the specimen to preserve three-dimensional anatomical relationships during curing. |
Wooden frame/stand, clear monofilament fishing line (2 kg test), fine sewing needles, clamps |
| 5. | Instructional planning and labeling schema:
Identify anatomical structures to be labeled (e.g., roots, trunks, cords, terminal branches) in alignment with curricular learning objectives prior to embedding. |
Label schema, anatomy checklist. |
| 6. | Label preparation:
Print clear adhesive labels with black text. Waterproof labels using a clear sealant spray and allow it to dry fully (≥24 hours). Pre-coat labels with a thin layer of epoxy resin to promote adhesion and prevent delamination during embedding. |
P-Touch PTD-220 (or equivalent), clear label tape, Gorilla Waterproof Patch and Seal Spray (crystal clear) |
| 7. | Epoxy resin selection:
Use Fiberglass Coatings™ “Superclear Table Top Epoxy,” selected based on prior trials for improved optical clarity and reduced exothermic reactivity. |
“Superclear Table Top Epoxy™” (two parts) |
| 8. | Preparation of mixing and inspection tools:
Assemble mixing tools, degassing equipment, and inspection aids, including a resin bubble remover or vacuum degassing device and a light pad positioned beneath the mold to enhance visualization of air entrapment. |
Manual mixing paddles preferred (for small amounts of resin); Resiners resin bubble remover; light pad (Toheto™ A4 rechargeable Light Pad). |
| 9. | Initial resin mixing and degassing:
Mix small batches of epoxy resin and hardener according to manufacturer instructions. De-gas the mixture for approximately 15 minutes, with additional 5-minute cycles as needed to reduce entrained air. |
Mixing cups, silicon paddles, timer, bubble remover/vacuum chamber |
| 10. | Base layer formation:
Pour a thin base layer of resin into the mold and allow it to partially cure until tacky. This layer stabilizes the specimen and prevents movement during subsequent pours. |
Mixed epoxy; mold; timer |
| 11. | Specimen pre-coating:
Apply two thin layers of epoxy resin to the specimen using a fine paintbrush. This step stabilizes tissue orientation and buffers neural structures against thermal effects during curing. |
Small paintbrushes; small beaker of mixed epoxy |
| 12. | Specimen positioning:
Position the pre-coated specimen onto the tacky base layer and adjust suspension lines to achieve the desired anatomical configuration. |
Suspension rig, forceps, hemostats |
| 13. | Incremental resin pours:
Pour resin in small increments of approximately 50 ml (<0.6 cm depth per pour) to minimize heat buildup. Allow brief intervals between pours as needed to maintain controlled curing. |
Measuring cups, bubble remover |
| 14. | Bubble detection and removal:
After each pour, inspect the resin surface using the light pad. Remove surface bubbles using a heat gun applied briefly and cautiously to avoid thermal damage. |
CALPALMY™ bubble-removing heat gun (5–10 min passes); scalpel for surface blisters |
| 15. | Layering progression:
Repeat incremental pouring and bubble removal until the mold reaches the desired depth (approximately 5 cm). |
Timer; log sheet for volumes/intervals |
| 16. | Label embedding:
Embed pre-coated labels during intermediate layers by placing them onto a tacky resin surface to prevent shifting or floating. |
Prepared waterproof labels; tweezers; small resin cup/brush |
| 17. | Curing conditions:
Allow the fully filled mold to cure undisturbed at room temperature for 48 hours. Avoid movement during curing to preserve anatomical orientation. |
Stable, level bench; ambient monitoring |
| 18. | Demolding and finishing:
Carefully remove the cured resin block from the mold, supporting the specimen to avoid shear stress. Sand sharp edges as needed to improve handling safety. |
Dust cover; cure log |
Intended Use and Scope
This optimized protocol is designed to produce durable, transparent, and pedagogically functional anatomical specimens suitable for repeated handling in educational settings. While developed using the brachial plexus as a test structure, the approach may be adapted to other anatomically complex regions with appropriate modification. Further refinement and comparative evaluation across additional specimen types and resin formulations remain areas for future investigation.
This study demonstrates the feasibility of developing epoxy-resin embedded human anatomical specimens through an iterative, trial-based methodological approach designed specifically for anatomy education. Rather than presenting a finalized or universal protocol, the work intentionally documents successive refinements in resin selection, suspension strategies, pour volumes, and de-bubbling techniques, highlighting how each modification addressed limitations identified in earlier trials. This approach reflects the practical realities faced by educators seeking to create durable, high-fidelity teaching tools under constrained institutional conditions.
Across the three trials, several methodological insights emerged as particularly consequential for preserving anatomical fidelity and instructional usability. Resin selection proved critical: while the initial epoxy formulation enabled baseline embedding, subsequent substitution with a lower exothermic, higher-clarity epoxy substantially improved optical transparency and reduced tissue distortion. Similarly, the transition from rudimentary suspension methods to a monofilament fishing-line system allowed more consistent maintenance of three-dimensional anatomical relationships, a feature especially important for complex neuroanatomical structures, such as the brachial plexus. These refinements underscore that anatomical orientation is not merely a technical consideration, but a pedagogical one, directly influencing the educational value of the resulting specimen. Incremental resin pouring and enhanced de-bubbling strategies further reduced exothermic effects and air entrapment, addressing common challenges reported in prior epoxy embedding studies. Importantly, these refinements were implemented using commercially available tools and materials, supporting the feasibility of in-house specimen development without specialized facilities. The addition of specimen pre-coating and integrated labeling in the final trial further enhanced stability and instructional clarity, aligning the physical specimen with curricular learning objectives and active learning environments.
Compared with previously described resin embedding protocols, which often prioritize display quality, archival preservation, or whole-organ visualization, the present study emphasizes protocol development as a transparent process rather than an end-state outcome. By explicitly reporting procedural challenges alongside successful refinements, this work provides educators with actionable guidance for troubleshooting common embedding issues, an aspect that is often underrepresented in the literature. In this way, the study complements existing preservation-focused approaches while addressing a distinct educational need.
Limitations
Several limitations warrant consideration. Access to human donor material remains a fundamental constraint for many institutions, limiting scalability and reproducibility across settings. Additionally, only two epoxy resin formulations were evaluated, and the long-term durability and optical stability of the resulting specimens have not yet been assessed beyond the initial implementation period. While the brachial plexus served as an effective test structure due to its anatomical complexity, further evaluation across additional regions and tissue types is necessary to determine the broader applicability of the protocol. Future studies should also investigate learner perceptions and educational outcomes associated with the use of epoxy-embedded specimens in comparison with plastinated materials, digital resources, and traditional human donor exposure. Despite these limitations, the findings highlight the value of iterative methodological refinement in developing teaching-oriented anatomical specimens. By aligning technical decisions with educational priorities, this approach supports the creation of accessible, durable resources that extend learning beyond the dissection laboratory and enhance engagement in active learning contexts.
An additional limitation relates to outcome assessment. Evaluation of optical clarity, anatomical positioning, structural integrity and pedagogical usability was performed using structured qualitative criteria rather than a quantitative approach. While this approach was appropriate for the development of practice-oriented goals of the project, it limits the ability to provide objective comparisons across resin formulations or protocols. Future work could incorporate objective measures, such as light transmittance to quantify optical clarity, for example, as well as formal user-testing protocols to evaluate educational effectiveness.
A further limitation concerns the assessment of educational utility. Although the specimens were reviewed for instructional practicality, this evaluation was conducted exclusively by faculty and did not involve student users or formal classroom implementation. Consequently, positive suggestions for “educational use” should be interpreted as preliminary judgements about usability and instructional potential rather than evidence of improved learning. Future studies should incorporate structured student-centered evaluations, including usability testing, learner feedback, and comparisons of educational outcomes between traditional and epoxy-embedded specimens.
This study presents an iterative, trial-based framework for developing epoxy-resin embedded human anatomical specimens tailored to anatomy education. Through systematic refinement across three sequential trials, the final protocol achieved improved optical clarity, anatomical stability, and pedagogical usability while remaining accessible to institutions with limited resources. By foregrounding methodological transparency and instructional intent, this work offers a reproducible approach for educators seeking to expand hands-on anatomical teaching tools beyond the dissection laboratory. Rather than proposing a universal solution, the protocol is intended as a flexible foundation that can be adapted to different anatomical regions, human materials, curricular goals, and institutional contexts. Continued refinement and educational evaluation will be essential to further optimize epoxy embedding as a teaching strategy. Nonetheless, this work demonstrates that purposeful, iterative protocol development can yield high-fidelity, cost-effective anatomical specimens that meaningfully support contemporary anatomy education.
ACKNOWLEDGEMENTS
The authors extend their deepest gratitude to individuals who generously donated their bodies to science, enabling anatomical education and research. The knowledge gained from these gifts advances scientific understanding and contributes to improved patient care. These donors and their families are honored with the utmost respect and appreciation.
Azer SA, Eizenberg N. 2007: Do we need dissection in an integrated problem-based learning medical course? Perceptions of first- and second-year students. Surg Radiol Anat 29(2):173-180.
https://doi.org/10.1007/s00276-007-0180-x
Burgess A, Bleasel J, Haq I, Roberts C, Garsia R, Mellis C. 2017: Team-based learning (TBL) in the medical curriculum: better than PBL? BMC Med Educ 17: 243-254. https://doi.org/10.1186/s12909-017-1068-z
Burgess A, Van Diggele C, Roberts C, Mellis C. 2020: Team-based learning: design, facilitation and participation. BMC Med Educ 20(S2): 461- 468. https://doi.org/10.1186/s12909-020-02287-y
Silva Cadete Tomás KDP, Silva MR, Garcioix VN, Giacometti LNW, Ramos Cardoso VG, Santos de Matos J, Magnani Branco BH, França Garcia, L, Pavanello A, Da Costa KM. 2025: Applications of 3D printing in the teaching of human anatomy: An integrative review. Ann 3D Print Med 19: 100213.
https://doi.org/10.1016/j.stlm.2025.100213
Drake RL, Vogl W, Mitchell AWM. 2023: Gray's Anatomy for Students. 5th ed. Elsevier.
Estai M, Bunt S. 2016: Best teaching practices in anatomy education: a critical review. Ann Anat 208: 151-157.
https://doi.org/10.1016/j.aanat.2016.02.010
Henry RW, Nel PP. 1993: Effects of dehydration mediums and temperature on total dehydration time and tissue shrinkage. J Plastination 7(1): 14-21. https://doi.org/10.56507/XNQM4606
Holliday SD, Blaylock BL, Smith BJ. 2001: Risk Factors Associated with Plastination: 1. Chemical Toxicity Considerations. J Int. Soc. Plast 16: 9-13. https://doi.org/10.56507/CWZW6925
Johnson C. 2009: Team-Based Learning for Health Professions Education: A Guide to Using Small Groups for Improving Learning. J Chiropr Educ 23(1): 47-48.
Latorre RM, García-Sanz MP, Moreno M, Hernández F, Gil F, López O, Ayala MD, Ramírez G, Vázquez JM, Arencibia A, Henry RW. 2007: How useful is plastination in learning anatomy? J Vet Med Educ 34(2): 172-176.
https://doi.org/10.3138/jvme.34.2.172
Lazarus MD, Chinchilli VM, Leong SL, Kauffman GL. 2012: Perceptions of anatomy: critical components in the clinical setting. Anat Sci Educ 5(4): 187-199. https://doi.org/10.1002/ase.1270
Liaison Committee on Medical Education (LCME). 2024: Functions and Structure of a Medical School: Standards for Accreditation of Medical Education Programs Leading to the MD Degree. Association of American Medical Colleges.
Hashida K, Shirakhata K, Thompson J, Liang C, Takakusagi M, Stenger K, Lozanoff BK, Labrash S, Rettenmeier C, Gestewitz M, Lee U-Y, Doll S, Lozanoff S. 2021: Plastinated instructional assets utilization during collaborative online head and neck anatomy in the medical education. J Plastination 33: 28-38.
https://doi.org/10.56507/KDHJ2784
McMenamin PG. 2008: Body painting as a tool in clinical anatomy teaching. Anat Sci Educ 1(4): 139-144.
https://doi.org/10.1002/ase.26
Netter FH. 2022: Atlas of Human Anatomy. 8th ed. Elsevier.
Parmelee D, Michaelsen LK, Cook S, Hudes PD. 2012: Team-based learning: a practical guide: AMEE Guide No. 65. Med Teach 34(5): e275-e287. https://doi.org/10.3109/0142159X.2012.651179
Pirici I, Cercelaru L, Stanca DI, Osman A, Sas L, Pirici D, Mindrilla I. 2023: Simple Universal Whole Organ-Resin Embedding Protocol for Display of Anatomical Structures. Biomedicines 11: 1433.
https://doi.org/10.3390/biomedicines11051433
Ravi SB, Bhat VM. 2011: Plastination: A novel, innovative teaching adjunct in oral pathology. J Oral Maxillofac Pathol 15(2): 133-137. https://doi.org/10.4103/0973-029X.84475
Reimschisel T, Herring AL, Huang J, Minor TJ. 2017: A systematic review of the published literature on team-based learning in health professions education. Med Teach 39(12) 1227- 1237.
https://doi.org/10.1080/0142159X.2017.1340636
Sora MC, Matusz P. 2012: Study of the vascular architecture of bones using the plastination technique. Clin Anat 25(2): 258-259. https://doi.org/10.1002/ca.21271
Sugand K, Abrahams P, Khurana A. 2010: The anatomy of anatomy: a review for its modernization. Anat Sci Educ 3(2): 83-93. https://doi.org/10.1002/ase.139
Thiel W. 1992: Die Konservierung ganzer Leichen in natürlichen Farben [The preservation of the whole corpse with natural color]. Ann Anat 174(3): 185-195. https://doi.org/10.1016/S0940-9602(11)80346-8
Turney BW. 2007: Anatomy in a modern medical curriculum. Ann R Coll Surg Engl 89(2): 104-107.
https://doi.org/10.1308/003588407X168244
Vasan NS, DeFouw DO, Compton S. 2011: Team-based learning in anatomy: an efficient, effective, and economical strategy. Anat Sci Educ 4(6): 333-339. https://doi.org/10.1002/ase.257
Von Hagens G, Tiedemann K, Kriz W. 1987: The current potential of plastination. Anat Embryol (Berl) 175(4): 411-421. https://doi.org/10.1007/BF00309669
Winklemann A. 2007: Anatomical dissection as a teaching method in medical school: a review of the evidence. Med Educ 41(1): 15-22. https://doi.org/10.1111/j.1365-2929.2006.02625.x