1Department of Medical Education, College of Medicine & Life Sciences, University of Toledo, Toledo, Ohio, USA
2Department of Chemistry, College of Natural Sciences and Mathematics, University of Toledo, Toledo, Ohio, USA
3Department of Neurobiology & Anatomy, College of Medicine, Drexel University, Philadelphia, Pennsylvania, USA
Finding efficient ways to plastinate specimens has the potential to increase production capacity and reduce costs, thereby benefiting the learning community. This study focused on human brain tissue due to its delicate structure and high demand in neuroanatomy education. Eleven human brains were sectioned into approximately 5 mm slices in both coronal and transverse planes. Ten specimens were stained using either Le Masurier’s Method (Prussian Blue Reaction) or Alston’s Method, while one specimen remained unstained. Following cold-temperature dehydration (-25°C) in acetone, all specimens were impregnated using a standard cold-temperature silicone mixture at room temperature. Measurements were recorded prior to staining and after the completion of curing. The average shrinkage across all slices was 8.9 ± 4%, and the overall processing time was reduced compared with traditional cold-temperature impregnation protocols. No significant differences in shrinkage were observed based on staining method or plane of section. Additionally, the incorporation of histological staining did not adversely affect the plastination process or the specimens' dimensional stability. These findings suggest that using cold-temperature silicone at room temperature enables more rapid impregnation, likely due to its lower initial viscosity, while maintaining shrinkage rates comparable to those of traditional methods. This supports the concept that early-phase polymer infiltration plays a critical role in minimizing tissue distortion despite time-dependent increases in viscosity. Overall, room-temperature plastination represents a practical, resource-efficient alternative for producing high-quality neuroanatomical teaching specimens.
Alston’s method; brain: Le Masurier’s method; room temperature; shrinkage; silicone; S10; S3
John Cichewicz, Department of Medical Education, University of Toledo College of Medicine and Life Sciences, Toledo, OH 43614 USA
e-mail: jcichewicz00@gmail.com

![]()



Plastination is the process of using polymers (such as silicone, epoxy, or polyester) to create permanent models from once-perishable specimens, producing highly accurate anatomical specimens for teaching purposes (Sagoo & Adds, 2013). The standard cold-temperature silicone plastination technique can be expensive to perform because it requires deep freezers (-25°C) for dehydration and impregnation. Obtaining a freezer capable of maintaining such a low temperature can be costly (Sagoo & Adds, 2013; Starchik & Henry, 2015). This is especially true if the specimen of choice is large or if numerous pieces need to be preserved at once. The other factor hindering production is the time required for impregnation. At low temperatures, impregnation is a slow process and can take several weeks (Starchik & Henry, 2015). The longer it takes for specimens to finish, the more the lab’s ability to plastinate additional specimens is limited for a considerable period. This combination of a slow process and limited space truly limits the number of specimens that can be produced at a time, especially for newly founded labs.
There is currently a widely accepted room-temperature plastination method that uses a different silicone-crosslinker mixture (Henry 2007). The silicone and crosslinker for room-temperature plastination are reactive with the silicone and hardener used for cold-temperature plastination, meaning that the chemical requirements can be counterproductive if cross-contamination occurs (Starchik & Henry, 2015). Said cross-contamination can cause specimens to become trapped in solid blocks of silicone before proper impregnation occurs. To avoid this, there must be ample space if a laboratory wishes to perform both processes. This extra set of silicone products can take up valuable space in small labs. Aside from those limitations, the hardening process of the room-temperature plastination method can take months or even years in large specimens. Compared to the cold-temperature method, this hardening process on larger specimens is long and slow, and repeated applications may be necessary (Starchik & Henry, 2015).
There has been research on how room-temperature plastination compares with the standard cold-temperature method, but both techniques are still needed. Starchik and Henry (2015) calculated the shrinkage of many specimens that had undergone the standard cold-temperature plastination method and the standard room-temperature plastination method. In all tissue types they tested, specimens from the room-temperature trials exhibited less shrinkage and were completed in less time (Starchik & Henry, 2015). This means that the room-temperature method resulted in less shrinkage and a more accurate final product. Although this information suggests that the room-temperature method is better, there is still a need for the cold-temperature process. Different temperature plastination techniques are better suited to different types of specimens due to differences in silicone viscosity and shrinkage between the two standard methods (Starchik & Henry, 2015). This means that a laboratory aiming to produce a variety of specimens needs to be able to perform both cold- and room-temperature plastination.
Several groups have tested room-temperature methods and hybrid workflows that pair low-temperature dehydration with room-temperature impregnation, reporting practical advantages for lab use. Room-temperature impregnation with Biodur S10/S3 mixtures produces durable, easy-to-handle brain specimens for teaching while reducing equipment demands and the high capital costs of continuously running ultra-low freezers (De Jong & Henry, 2007; Mooncey & Sagoo, 2014; Ottone et al., 2015). Beyond cost, room-temperature workflows also reduce the safety risks associated with storing acetone in non-spark-proof freezers, as Zheng et al. (1998) highlighted. This minimizes the risk of explosion due to the interaction between acetone fumes and the freezer's motor ignition (Gubbins, 1990; Zheng, 1998; Ottone et al., 2015). Taken together, the cost savings, improved safety, and reports of preserved surface detail and teaching quality make a strong case for controlled studies on how impregnation temperature affects shrinkage in delicate brain tissue.
Research by Henry (2008) has shown that room-temperature plastination can be done using cold-temperature silicone. They concluded their research by stating that the quality of the specimens was lower than the “gold standard” but high enough for teaching. Similar to Sagoo and Adds (2013), our lab group performed a preliminary experiment that involved preserving stained brain slices at room temperature using the cold-temperature method. The conclusion drawn from the preliminary research was that using the cold-temperature method at room temperature resulted in slight shrinkage in the samples and faster impregnation. It was also noted that the specimens were of high enough quality for instruction, consistent with Henry’s data.
The goal of this experiment was to determine whether using cold-temperature silicone to plastinate brain specimens at room temperature would yield finished specimens with comparable shrinkage to those made using the standard cold-temperature method. If this is concluded, the use of delicate brain tissue specimens would apply to other types of specimens as well. It could be a proposed method for laboratories producing plastinated specimens to produce them at a faster rate and at lower cost, as the need for a cold freezer to be operated for an extended period would not arise. It could eliminate the need for cold-temperature plastination or, at the very least, make it an optional method. The idea of saving time, space, and money is key for labs with limited space and a variety of specimen types to plastinate for teaching purposes.
Preparation of Specimens & Staining
Figure 1. The measuring grid used for the surface area calculation of brain slices
Eleven whole-brain specimens (6 female, 5 male; age range 74–89 years) were obtained from donors who had been embalmed via the carotid and femoral arteries at room temperature (71 °F (21.67 °C; ~15% humidity) using an embalming solution consisting of 42% ethyl alcohol, 23% of 37% formaldehyde, 15% of 90% phenol, 14% ethylene glycol, 14% glutaraldehyde, and 16% EDTA, diluted 1:2 with water. On post-embalming day three, the brains were removed from the donor and immersed in 10% formalin for a minimum of 6 months at room temperature prior to processing.
Specimens were cleared of arachnoid mater and vasculature using forceps and sectioned into 5-mm slices in either the transverse or coronal plane using a commercial deli slicer (Univex Model 4612). Prior to dehydration, the slices were imaged on a measurement grid for initial surface area analysis (Fig. 1). Following these measurements, specimens were returned to 10% formalin until staining commenced. For staining preparation, slices were rinsed in tap water for 2 hours and allocated as follows: five specimens stained using LeMasurier’s (Prussian blue reaction) method and five using Alston’s method (Fig. 2), with all protocols performed according to Suriyaprapadilok and Withyachumnarnkul (1997). One brain was left
 Figure 2a Brain slice after staining, but before plastination, showing LeMasurier’s Method |
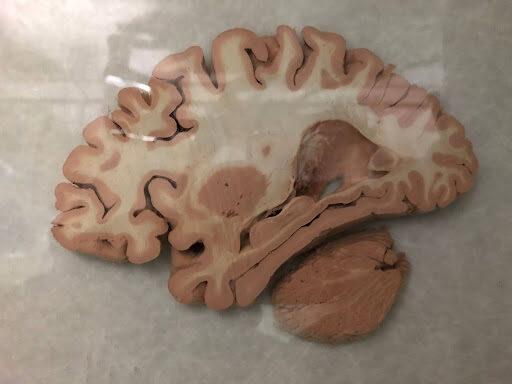 Figure 2b Brain slice after staining, but before plastination, showing Alston’s Method. |
unstained to serve as a control. After staining, specimens were rinsed under running water for 8 hours (Fig. 3) and secured using a metal grid “sandwich method” to maintain flatness and structural integrity during processing (Fig. 4). The secured grids were then transferred directly to the dehydration phase (Fig. 5). To properly track each section during this process, the grids were numbered following staining and prior to dehydration and were transferred directly to impregnation afterwards. They were taken out of the ‘sandwich’ after impregnation, but before curing. They were organized by placing each section on an individual tray with its corresponding numbered grid during curing.
 Figure 3. Water bath used for cleaning specimens following staining and before plastination |
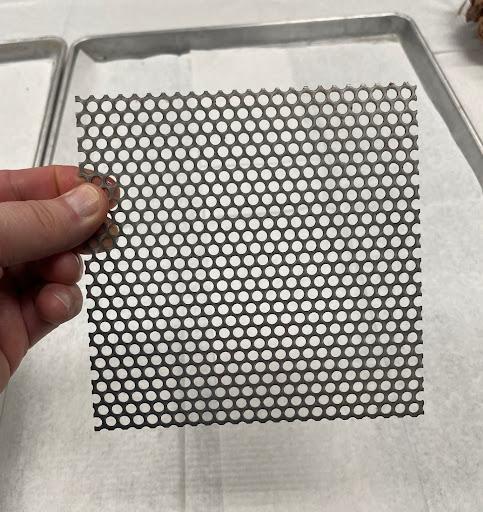 Figure 4. Image of a single metal grid used for the stacking of brain slices |
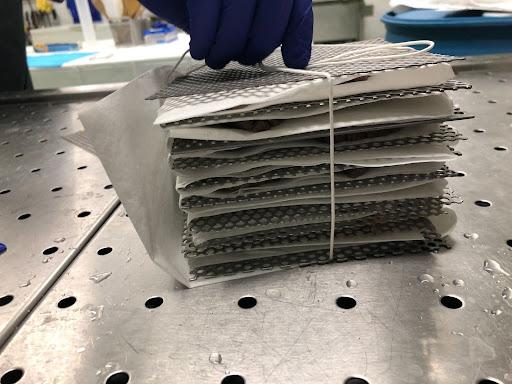 Figure 5. Application of metal grids and paper towels in successive stacking for dehydration |
Dehydration
The stained and rinsed specimens were dehydrated at -20 °C using acetone (100%). Once a week, the specimens were transferred into new 100% acetone. The purity of acetone was monitored using an acetonometer calibrated to 20 °C. The specimens were considered dehydrated when the acetone purity remained above 99.5%. This took 3 rounds of 100% cold acetone 10:1.
Impregnation
The specimens were then transferred directly from cold acetone to the room-temperature vacuum impregnation chamber containing the same S10:S3 polymer mixture (100:1) as in the traditional von Hagens method. Impregnation was initiated upon transfer to silicone and lasted for 17 days at room temperature (20 °C) without any deactivation periods. After reaching 10 mmHg with little to no bubbling in the silicone surface mixture, the impregnation was considered completed, and all specimens were raised from the silicone to drain inside the chamber.
Figure 6. The measuring grid is being used to calculate the surface area of the brain slice
After draining at room temperature, the specimens were hardened using vaporized S6 for 6 days. The remaining silicone was returned to the freezer (-25 °C) for preservation. The impregnation protocol was modified from Sora (2016) by changing only the impregnation temperature.
Imaging
After completing the hardening process, specimen slices were imaged using a pane of glass and a 1 mm control grid (Figs. 1 and 6) in the same method as discussed prior to the plastination process. Five representative slices were selected from each specimen: three from the center (center slices, CS) and one from each edge (edge slices, ES), to streamline data collection and analysis. Selected slices were manually traced using ImageJ, an open-source image processing and analysis software developed by the National Institute of Health and implemented in Java. The control grid included in each photograph enabled software calibration to ensure accurate measurements. Following calibration, changes in surface area were quantified by tracing brain images at each stage. Tracing and measuring were performed by the same researcher to prevent inter-rater reliability issues.
The average shrinkage of the 5 representative slices (CS+ES) in regard to gray matter and white matter is shown in Table 1. The percentage of shrinkage was calculated by subtracting the post-plastination area measurement from the pre-plastination area measurement, dividing the difference by the pre-plastination area, and multiplying by 100. The average for each measured slice is shown with its standard deviation to better interpret the results. The average shrinkage of each slice according to the plane of dissection is shown in Table 2. There is no difference in measurements between transverse and horizontal slices, indicating that the slice plane had no discernible influence on slice shrinkage. The average slice shrinkage for each stain is shown in Table 3. No staining method influenced the shrinkage.
| Average (%) | Standard Deviation | |
| Slice Shrink | 8.893 | ±4.327 |
| White Matter Shrink | 20.514 | ±6.186 |
| Gray Matter Shrink | 2.063 | ±7.562 |
| Average (%) | Standard Deviation | |
| Transverse | 8.665 | ±5.078 |
| Coronal | 9.121 | ±3.59 |
| Average (%) | Standard Deviation | |
| Alston | 10.292 | ±5.012 |
| La Masurier | 7.527 | ±3.656 |
| None | 10.195 | ±4.289 |
The shrinkage of gray and white matter was not consistent, with white matter exhibiting more pronounced contraction (Table 1). One explanation could be that white matter has a higher fat content due to a higher concentration of myelin (the sheath of axons). Gray matter has much less fat content, as it is composed of cell bodies and has significantly fewer oligodendrocytes (lining axons). Acetone acts as a defatting agent, even at -20 °C (Dezse et al., 2020); the resulting lipid extraction leads to greater volume loss in white matter compared to gray matter, which is primarily composed of cell bodies and contains fewer oligodendrocytes (Sora, 2016).
Our results showed an average brain slice shrinkage of 8.89% (range 4.6-13.2%). This aligns with Suriyaprapadilok and Withyachumnarnkul (1997), who reported approximately 9% shrinkage in 5 mm brain slices using cold-temperature impregnation. During this stage, rapid acetone removal can cause shrinkage if the silicone polymer does not replace the solvent at a comparable rate (Weiglein, 1996). Our findings suggest that cold-temperature silicone protocols performed at room temperature yield results comparable to traditional cold-temperature processing. While Brown et al. (2002) identified shrinkage as a primary drawback of room-temperature plastination in nervous tissue, our results align with Ottone et al. (2015), who observed minimal morphological changes using a cold silicone mixture at room temperature. Furthermore, the plane of section did not significantly influence shrinkage (Table 2), which is congruent with the findings of Starchik and Henry (2015). This suggests that shrinkage may be more strongly influenced by temperature and protocol than by the components of the silicone mixture.
This apparent discrepancy in the literature may be explained by the dynamic relationship between temperature, viscosity, and time during impregnation (Sora, 2017; Monteiro et al., 2018). Although room temperature conditions initially reduce silicone viscosity and may enhance early tissue penetration, viscosity increases progressively over time due to ongoing polymer chain extension, thereby narrowing the effective working window (Adds, 2017; Sora, 2017). In contrast, cold-temperature impregnation maintains a higher but more stable viscosity throughout the process (Sora, 2017). Thus, room temperature plastination may offer an early-phase advantage in polymer infiltration but introduces time-dependent variability that can limit penetration if not carefully controlled (Adds, 2017). These findings suggest that successful room-temperature plastination depends not only on temperature but also on maintaining an appropriate balance between viscosity and impregnation duration to ensure adequate polymer replacement of acetone (Monteiro et al., 2022).
In addition to the role of viscosity during impregnation, the curing phase represents a critical but often underemphasized step in plastination. Curing, typically achieved by exposure to a crosslinking agent such as S6 vapor, stabilizes the silicone polymer and preserves the specimen's final anatomical configuration. Importantly, prior work suggests that curing itself is not a primary contributor to tissue shrinkage; rather, it serves to “lock in” the dimensional changes that occur during dehydration and forced impregnation (Monteiro et al., 2022). This distinction reinforces the conclusion that the comparable shrinkage observed in this study is most likely attributable to improved early-phase polymer infiltration under lower-viscosity, room-temperature conditions, rather than to differences in the curing process. In the present study, the use of a cold-temperature silicone system (S10/S3) at room temperature permitted vapor-phase curing with S6, rather than the wipe-on curing methods commonly used in traditional room-temperature plastination protocols. Vaporized curing agents provide more uniform penetration and crosslinking of the silicone polymer, which may contribute to more consistent hardening and reduced processing time. While curing is not a primary determinant of tissue shrinkage, the efficiency and uniformity of vapor curing likely enhanced overall workflow and specimen quality within this hybrid approach.
Additionally, our average shrinkage (≈8.9%) confirms that staining methods, such as Astra Blue or Aldehyde-Fuchsin, are compatible with room temperature plastination without compromising dimensional stability, as shown in Table 3 (Ulfig and Wuttke, 1990; Baeres and Møller, 2001). These hybrid methods offer operational advantages, including reduced equipment demands and safety risks, while providing faster impregnation times, making them well-suited for teaching laboratories (Zheng et al., 1998; Mooncey & Sagoo, 2014).
One specimen in the study had Parkinson’s disease; however, shrinkage did not differ from that of the other samples. Although pathogenicity was not the primary focus of the study, this incidental finding warrants consideration, particularly regarding how other pathologies—such as demyelinating disorders—may influence shrinkage outcomes.
This study did not include a formal control group due to time and financial limitations; instead, it builds on previously validated control designs reported by Suriyaprapadilok and Withyachumnarnkul (1997). To avoid redundant resource use, baseline controls were not repeated. Accordingly, the analysis focused exclusively on the effects of using a cold-temperature silicone mixture applied at room temperature on plastination-related specimen shrinkage, thereby maintaining methodological continuity with prior work. The absence of a parallel control group is acknowledged as a limitation; however, the study design is supported by robust historical control data from Suriyaprapadilok and Withyachumnarnkul (1997) and Ottone et al. (2015).
A key distinction between our study and that of Suriyaprapadilok and Withyachumnarnkul (1997) is the use of a cold-plastination silicone mixture at room temperature, similar to Ottone et al. (2015), which resulted in noticeably less tissue shrinkage. This effect was particularly evident in nerve tissue and is consistent with observations by Starchik and Henry (2015), who also reported diminished shrinkage at room temperature, although this was not their primary focus. Although room temperature is not a replacement for the cold-temperature method, our findings suggest it is a practical and effective alternative for select tissue types when reduced shrinkage, resource efficiency, or logistical flexibility is desired.
In summary, the use of a cold-plastination silicone mixture at room temperature was associated with reduced tissue shrinkage while maintaining structural integrity across specimens, with particularly favorable outcomes in nerve tissue. Although the absence of a parallel control group limits direct comparison, the findings align with established historical controls and prior observations in the literature. Together, these results support the feasibility of room-temperature plastination protocols as a practical and resource-conscious alternative in selected contexts. Future studies incorporating prospective control groups and a broader range of tissue types will be essential for refining best practices and validating reproducibility. Such work will inform the continued development of scalable plastination workflows and guide the implementation of dedicated plastination laboratory infrastructure to support education, research, and innovation.
This study demonstrates that using a room-temperature silicone mixture can produce plastinated brain specimens with shrinkage comparable to traditional cold-temperature methods while preserving structural integrity. The observed outcomes highlight the importance of viscosity as a central factor in plastination, governed by the interplay between temperature and impregnation time. While room temperature conditions may facilitate initial polymer penetration due to lower viscosity, time-dependent increases in viscosity necessitate careful control of the impregnation process to prevent incomplete infiltration and subsequent shrinkage. These findings support room-temperature plastination as a viable and resource-efficient alternative for select applications, particularly in educational settings, provided that protocol parameters are carefully managed. Further investigation incorporating controlled comparisons and a wider range of tissue types will be critical to optimizing protocols and expanding the applicability of this approach.
ACKNOWLEDGEMENTS
The authors sincerely thank those who donated their bodies to science, enabling anatomical research. Results from such research can increase mankind's overall knowledge, thereby improving patient care. Therefore, these donors and their families deserve our highest gratitude (Iwanaga et al, 2020).
We would also like to express our appreciation to Elizabeth ‘Beth’ Dalzell, supervisor of lab preparation, and Diane Durliat, director of the body donation program at UTCOMLS, for assisting us in these efforts and for ensuring the respectful preservation of donors.
Special recognition is due to Dr. Carlos Baptista for allowing the use of his laboratory and for his wisdom throughout this process.
Lastly, we would like to thank our fellow lab partners who participated in the brain staining process. Thank you, Trevor Rhyans, Melissa Curtis, Chase Carr, and Laney Baldwin.
Adds, PJ. 2017: Biodur® S10/S3 and S15/S3 at “Room Temperature”: a viscosity study. J Plast 29(1):15-18. doi: 10.56507/RNBU9088.
Baeres FMM, Møller M. 2001: Plastination of dissected brain specimens and Mulligan-stained sections of the human brain. Eur J Morphol 39(5):307–311. doi:10.1076/ejom.39.5.307.7167
Brown MA, Reed RB, Henry RW. 2002: Effects of Dehydration Mediums and Temperature on Total Dehydration Time and Tissue Shrinkage. J Int Soc Plastination. 17:28-33. doi: 10.56507/XNQM4606
De Jong K, Henry RW. 2007: Silicone plastination of biological tissue: cold-temperature technique—Biodur™ S10/S15 technique and products. J Int Soc Plastination 22:2–14. doi: 10.56507/QCZA2836
Dezse KE, Frank WP, Baptista C. 2020: Fat Removal during Acetone Dehydration and Defatting Phases of Plastination. J Plast 32(1). doi: 10.56507/MBJO3692
Gubbins RBG 1990: Design of a plastination Laboratory. J Int Soc Plastination 4 (1): 24-27. doi: 10.56507/ZXJT8319
Henry RW. 2007: Silicone Plastination of Biological Tissue: Room-temperature Technique, North Carolina Technique, and Products. J Int Soc Plastination 22:26-30. doi: 10.56507/FSNZ3092
Henry RW. 2008: Room-temperature impregnation with cold-temperature silicone products. J Int Soc Plastination 23:40–41. doi: 10.56507/QIDA3140
Iwanaga J, Singh V, Takeda S, Kusukawa J, Matsushita T, Tubbs RS, et al. 2021: Acknowledging the use of human cadaveric tissues in research papers: Recommendations from anatomical journal editors. Clin Anat. 34:2–4. doi: 10.1002/ca.23671
Le Masurier M. 1987: The staining of cerebral slices by Astra blue and aldehyde fuchsin, and their subsequent plastination. Acta Anat (Basel) 128(1):59–61. doi: 10.1159/000146374
Monteiro YF, Juvenato L da S, Bittencourt AP, Siqueira B, Montiero FC, Baptista CAC, Bittencourt AS. 2018: Influence of the temperature on the viscosity of different types of silicone. J Plast 30(1). doi: 10.56507/HETT9088
Monteiro YF, Juvenato L da S, Bittencourt APSV, Baptista CAC, Bittencourt AS. 2022: Influence of silicone viscosity on shrinkage during room and cold temperature impregnation. J Plast 34(1). doi: 10.56507/AVGH6759
Mooncey MS, Sagoo MG. 2014: Comparative staining methods with room temperature plastination (15–18°C) of brain specimens, using Biodur™ S10/S3. J Plast 28:27–30. doi: 10.56507/TFQH5165
Ottone NE, Cirigliano V, Bianchi HF, Medan CD, Algieri, RD, Brum GB et al. 2015: New contributions to the development of a plastination technique at room temperature with silicone. Anat Sci Int 90:126–135. doi: 10.1007/s12565-014-0258-6
Sagoo MG, Adds PJ. 2013: Low-temperature dehydration and room-temperature impregnation of brain slices using Biodur™ S10/S3. J Plast 21(1):3–8. doi: 10.56507/TFQH5165
Sora MC. 2016: The general protocol for the S10 technique. Res Clin Med 1:14–18.
Sora MC. 2017: Room temperature Impregnation with Cold Temperature Biodur® Silicone: A Study of Viscosity. J Plast 29(1). doi: 10.56507/QIDA3140
Starchik D, Henry RW. 2015: Comparison of cold and room temperature silicone plastination techniques using tissue core samples and a variety of plastinates. J Plast 27:13–19. doi: 10.56507/NTQJ7764
Suriyaprapadilok L, Withyachumnarnkul B. 1997: Plastination of stained sections of the human brain: comparison between different staining methods. J Int Soc Plastination. 12:27–33. doi: 10.56507/YISQ6047
Ulfig N, Wuttke M. 1990: Plastination of stained sections of the human brain. Anat Anz. 170(4):309–312. doi: 10.1016/S0940-9602(11)80294-2
Von Hagens G. 1986: Heidelberg plastination folder: Collection of all technical leaflets for plastination. Biodur Products 2nd Edition
Weiglein AH. 1996: Preparing and using S-10 and P-35 brain slices. J Int Soc Plastination 11:6–10. doi: 10.56507/IXGV4189
Zheng TZ, Liu JR, Zhu KM. 1998: Plastination at room temperature. J Int Soc Plastination 13:21–25. doi: 10.56507/GJQQ9836