Institut fur Anatomie, Karl-Franzens-Universitdt Graz, Harrachgasse 21, A-8010 Graz, Austria, Europe
Tendon sheaths are complex tubes wrapped completely around tendons. They are placed between two movable tissues to diminish friction when tendons pass either under ligaments or retinacula or pass through fascial slings or osseofibrous tunnels. The aim of this study was to show that the El2 plastination technique is a useful research tool for demonstrating different anatomical structures, e.g. tendon sheaths in the talocrural region. Tendon sheaths were injected with Xantopren® blue and plastinated via the E12 plastination procedure. Finally, the cured specimens were cut with a diamond wire saw into slices of 200um thick. We found that tendon sheaths in the talocrural region do not enclose tendons like a cylinder. They mimic an elongated bursa that minimizes friction between tendons and retinacula.
sheet plastination; talocrural region; tendon sheaths
G. WINDISCH: Telephone: 43 316 380 - 4228 or 4215; Fax: 43 316 380- 9620; e-mail:

![]()



Tendon sheaths are similar to bursae in structure. They develop in response to friction between tendons and bones or tendons and ligaments, or fascial slings (Hartman, 1896). Bursae are closed connective tissue sacs underlying a tendon and can easily be converted into a tendon sheath simply by extension around the tendon. Hence, tubes are formed which wrap completely around tendons and consist of two layers. The structure of the fibrous layer shows a tight collagenous tissue that encloses the tendon like a tube. Therefore, it is able to reduce friction against bones (Hollinshead and Rosse, 1985). In the area of the tendon sheaths of fingers and toes, the outer layer has compact fibers surrounding the tendon called cruciate or annular ligaments.
The synovial surface is a closed double-walled cylinder and consists of two layers. The visceral layer is closely attached to the surface of the tendon. The second layer, surrounding the cavity, is known as the parietal layer. These two smooth, glistening layers, for the most part are separated from each other by synovial fluid and are continuous with each other at the end of tendon sheaths (Lovell and Tanner, 1908).
The best medium to produce ideal conditions for slicing plastinated specimens with a diamond saw is the epoxy (El 2, Biodur™) plastination technique. Xantopren® blue was chosen to inject the tendon sheaths due to its fluid nature. Xantopren® blue cures without damaging the sheath and does not shrink. These slices become translucent and provide detailed information about anatomical structures (McNiesh and von Hagens, 1988) in the talocrural region. Furthermore, with the thin slices, we were able to visualize tissue differences with the naked eye (Cook and Al-Ali, 1997; Skalkos et al., 1999). Also, tendon sheath structure was found to be different from classic descriptions.
Xantopren® blue (Bayer Dental, D-5090, Leverkusen, Germany) is used by dentists to get an impression of teeth to fit dental braces. Before starting the plastination procedure with El2, the compatibility of Xantopren® blue was checked by placing 10 ml Xantopren® blue into two containers. Fifty milliliters of acetone was added to one container and 50 ml of epoxy resin was added to a second. These mixtures were left together for 1 month to confirm the compatibility of Xantopren® blue with the E12 technique (Biodur™).
Five feet from human cadavers, aged between 34 and 76 years, were studied. All of the cadavers were embalmed by Thiel's method (Thiel, 1992). Dissection layer by layer was performed until the deep fascia of the leg and the dorsal fascia of foot were reached. Using a 10 ml syringe and a small needle, a mixture of Xantopren® blue and hardener [elastomer activator (Bayer Dental, D-5090, Leverkusen, Germany)] was injected into the upper end of the sheaths of the tibialis posterior m., extensor digitorum longus m. and flexor hallucis longus m. where the muscle fibers join the tendon. This must be done very precisely and with low pressure to avoid damage to the sheath. It also must be done quickly, to prevent the Xantopren® blue-hardener mix from curing within the syringe.
To be certain that only tendon sheaths were injected, and not fibers of the tendon or the surrounding loose peritendineum, our injections were verified with standard histology sections (Figs. 1, 2). Five human feet were prepared for routine histological examination. Tandler gelatin was injected via a 10 ml syringe and small needle into the tendon sheaths of the above mentioned muscles. Specimens were dehydrated in a graded alcohol series from 60% to 100% over a five- week period. All specimens were embedded in paraffin. Histological sections of 13 to Hµ™ were cut and evaluated.
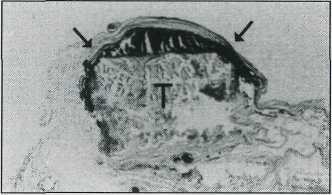 Figure 1. Histological section through a single tendon. Arrows showing Tandler gelatin injected tendon sheath, T - Tendon. |
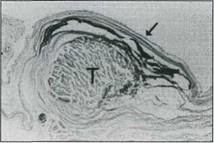 Figure 2. Histological section through a single tendon. Arrows showing Tandler gelatin injected tendon sheath, T- Tendon. |
Freezer and Band saw:
Feet with injected tendon sheaths were put into a freezer at -70°C for three days. Two-centimeter thick frontal sections were made with the band saw. To prevent warming of the specimen and slices, the band saw was equipped with a cooling chamber filled with cold water and bottles of frozen glycerine.
Dehydration and degreasing:
Cold acetone (-25°C) was used for dehydration. Water content was monitored regularly with the acetonometer. After three weeks, water content had decreased to 2% (purity of acetone 98%) and dehydration was deemed complete. To ensure extraction of lipids, degreasing in room temperature acetone was carried out for two weeks.
Immersion, impregnation and embedding:
The dehydrated slices were immersed into a mixture of Biodur™ E12 (epoxy resin) and Biodur™ E6 (hardener) (18%) over night for 12 hours. The specimens, in the original resin, were placed in the vacuum chamber and sealed with a glass plate. The slices were impregnated under vacuum ranging from 100 - 10mm Hg for 24 hours at -4°C. Pressure was monitored with a manometer. For embedding, slices were placed into a plastic form. The form was filled with a mixture of E12 and E6. To prevent them from floating and drifting, Plexiglas® plates were laid on the slices. Trapped bubbles were removed with a fine wire.
Pre-curing and curing:
It took one day for the epoxy resin to gelate at room temperature. The plastic form with the slice was cured in an oven for 48 hours at +45°C.
Band saw and diamond wire saw:
The plastic form with cured specimen was sawed into pieces measuring 7 x 15 cm. The pieces were fixed with plastic screws on blocks of wood in readiness for the diamond wire saw. This saw is equipped with a special bath filled with a mixture of water and petroleum to prevent the wire from gumming up with resin dust. The blocks were clamped on the guiding table and 200µm thick slices were made.
After one month, Xantopren® blue showed no reactivity with either acetone nor epoxy polymer. For our plastination project, Xantopren® blue proved to be an excellent material. As well as being compatible with the El2 polymer and acetone, it was fluid enough to inject into the tendon sheaths and fill them without damage. The translucent nature of these slices combined with the Xantopren® blue mass enabled differentiation of the various tissues and spaces. The blue filled only the cavity between tendons and retinacula, as seen on the sections (Figs. 3 - 5). It should be noted that Xantopren® blue was confined to only one side of the tendon. None of the injected tendon sheaths demonstrated the typical double-walled cylinder type sheath.
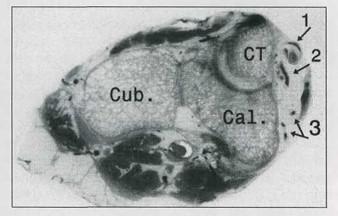 Figure 3. Frontal section through the collum tali (CT), calcaneus (Cal) and cuboid bone (CM) of right foot. Arrow 1 - Xantopren® blue injected tendon sheath of tibialis posterior muscle, Arrow 2 - Tendon sheath of flexor digitorum muscle. Both tendon sheaths lie on tendons, Arrow 3 - Vessels and nerve. |
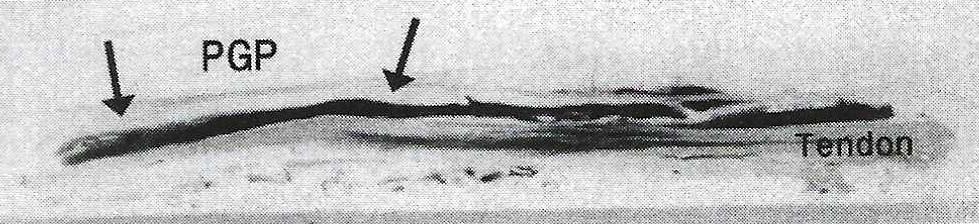 Figure 4. Sagittal section through a single tendon, |
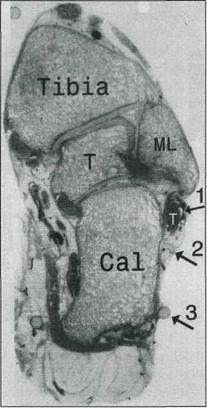 Figure 5. Frontal section through right ankle joint. Arrow 1 - Injected tendon sheaths, Arrow 2 - Flexor retinaculum, Arrow 3 - Plexiglas screw. T (white) - Tendon, T (black) - Tendon, ML - lateral malleolus. |
Histological sections showed tendon sheaths with Tandler gelatin lying on one side of the tendon like a pillow, hanging down with its corners to the medial and lateral side (Figs. 1, 2).
The aim of this work was to study the anatomy of synovial sheaths in the talocrural region by the use of the E12 plastination method as described by Weber and Henry (1993). The advantage of plastination is that plastinated slices preserve the relationship of one structure to another. With Xantopren® blue, we found a new material which proved to be very useful for this special plastination technique. Xantopren® blue was not reactive to the chemicals used in the E12 technique and filled the tendon sheaths without damaging them. Also, the 20(^m sections allowed us to distinguish dense connective tissue from loose tissue and to differentiate adjacent structures with the naked eye similar to the findings of Cook and Al-Ali (1997). The E12 technique may be used as an alternative method to the standard histological technique.
With the aid of the E12 plastination technique, we demonstrated a new method to delineate anatomical structures and function of tendon sheaths in the talocrural region. The results demonstrate that tendon sheaths of the tarsal region, indeed, show fundamental differences in the structure of the sheath from those usually embraced. These results were verified with standard histology sections, which showed that tendon sheaths are not wrapped completely around tendons (Figs. 1, 2). Since these tendons are held down by retinacula, the friction occurs between the tendon and the retinacula. Therefore, sheaths develop just in between these two movable tissues.
Cook P, Al-Ali S. 1997: Submacroscopic Interpretation of Human Sectional Anatomy using Plastinated E12 Sections. J Int Soc Plastination 12(2): 17-27.
https://doi.org/10.56507/XICY2283
Hartman H. 1896: Die Sehnenscheiden und Synovialsacke des Fusses. Morphol Arbeit 5:241.
Hollinshead W, Rosse C. 1985: In: Textbook of Anatomy, 4th ed. Philadelphia: Harper and Row. p 19-20.
Lovell AGH, Tanner HH. 1908: Synovial membranes, with special reference to those related to the tendons of the foot and ankle. J Anat Physiol 42:415-432.
McNiesh LM, von Hagens G. 1988: The diagnostic imaging characteristics of plastinated anatomical specimens. J Int Soc Plastination 2(l):24-39.
https://doi.org/10.56507/RMEK8272
Skalkos E, Williams G, Baptista CAC. 1999: The E12 Technique as an Accessory Tool for the Study of Myocardial Fiber Structure Analysis in MRI. J Int Soc Plastination 14:8-21.
https://doi.org/10.56507/ZLPM3596
Thiel W. 1992: Die Konservierung ganzer Leichen in naturlichen Farben. Anatomischer Anzeiger 174:185- 195.
https://doi.org/10.1016/S0940-9602(11)80346-8
Weber W, Henry RW. 1993: Sheet plastination of body slices - E12 technique, filling method. J Int Soc Plastination 7:6-22.
https://doi.org/10.56507/EZGX2343