University of Rome "La Sapienza", Rome, Italy
An invasive apocrine carcinoma of the perineal glands, involving the anal canal, vagina and vulva was surgically removed from a 62 year-old woman. The specimen was plastinated and macroscopically sectioned serially. The sections were photographed and compared to CT images made prior to surgery to verify and support the accuracy of the clinical diagnostic images.
MRI; CT; Scan
Maurizio Ripani University of Rome "La Sapienza", Rome, Italy

![]()



An invasive apocrine carcinoma of the perineal glands, involving the anal canal, vagina and vulva was surgically removed from a 62 year-old woman. The specimen was plastinated and macroscopically sectioned serially. The sections were photographed and compared to CT images made prior to surgery to verify and support the accuracy of the clinical diagnostic images.
A CT study of a 62 year-old woman revealed a neoplasm involving the left ischiorectal fossa, with neoplastic encasement surrounding the left heme- circumference of the anal canal, invading through the subepithelial structures of the vulva and posterior wall of the vaginal canal. The tumor was classified clinically as a perianal mucous-secreting adenocarcinoma. The tumor was surgically removed along with the bilateral inguinal lymph nodes, and colostomy was performed. Plastic surgery of the perineal area was performed using a myocutaneous flap of the left gracilis muscle and a slip of the anterior abdominal wall.
After a biopsy was taken for grading the tumor, the specimen was immediately processed for plastination. Specimen was cleansed of blood and fecal material and immersed in running tap water for 6 hours. To avoid alteration of shapes or anatomic relationships, the specimen was suspended in a metallic net. Dehydration was performed by freeze substitution with acetone at - 25°C. The acetone concentration was checked daily and upgraded as necessary with 100% acetone. We agitated the acetone solution before checking its concentration. Dehydration was complete in 8 days when the acetone concentration remained steady at 100%. Forced impregnation was begun by emerging the specimen in a mixture of Biodur polymer (S-10) and the hardener (S-3). Vacuum was applied and increased at one hour intervals during the day. We increased the vacuum throughout the day but we did not further increase it during the night hours (vacuum pump on from 8 AM to 4 PM for safety). Impregnation was ended when pressure was steady near 15 mm Hg. Pressure was steady when bubbles on the polymer surface practically disappeared. The specimen was removed from the vacuum chamber and excess polymer mix was allowed to drain from the specimen. The surface of the specimen was manicured and the specimen cured initially by the gas cure (S-6). The specimen was then sectioned serially (thickness was from 5 mm to 15 mm) and both sides of the section were photographed using a Linof professional camera.
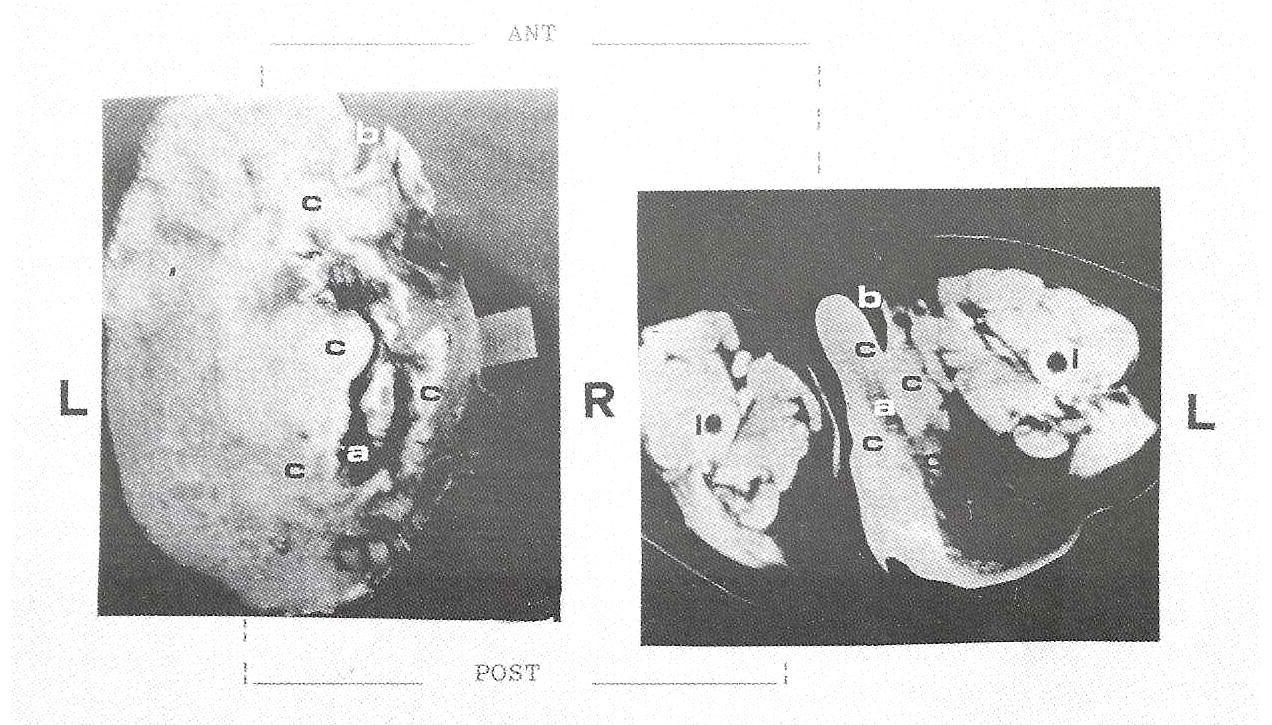
The neoplasm was a perianal mucinous adenocarcinoma. The plastinated specimen demonstrated the neoplasm invading the colon. The tumor distorted the normal morphology and rearranged the normal anatomic relationships (Fig. 1). Both the CT image and plastinated specimen placed the neoplasm in the left perineal area. The most caudal section of the plastinated specimen and CT image demonstrated the jagged outline of the tumor almost completely obstructing the rectal canal (Fig. 2,3).
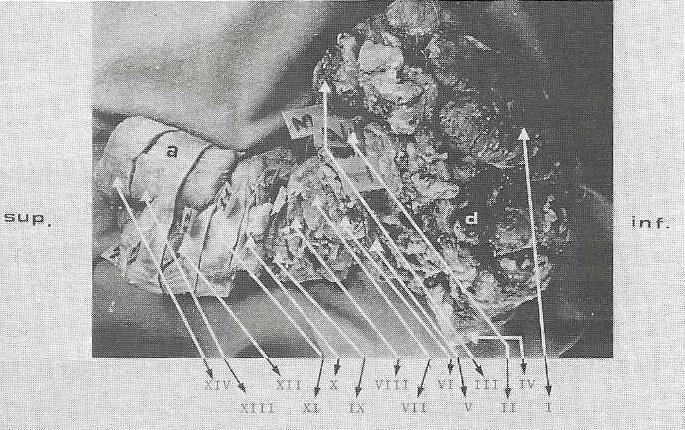 Figure 1.Right view of the surgical specimen |
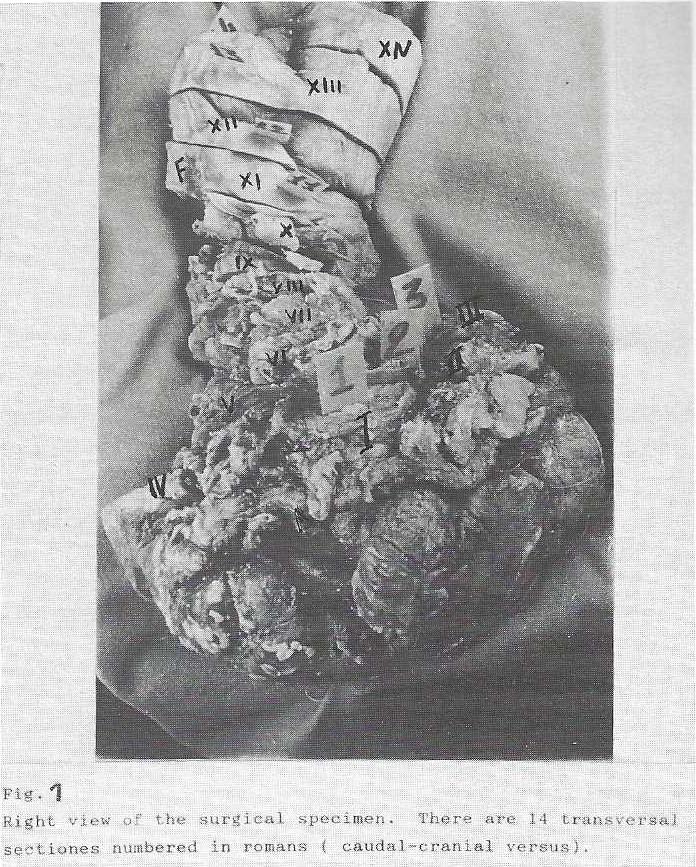 Figure 1. Righ view of the surgical specimen |
 Figures 2 and 3 |
|
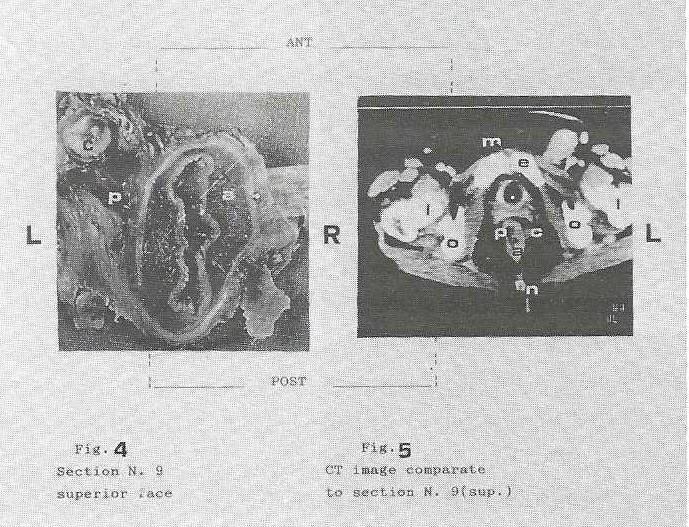
In the cranial (9th section) sections, the neoplasm was located perirectally with minor evidence of invasion of the rectal wall (Fig. 4) and CT images of (Fig. 5 ) the prerectal and perirectal vessels were disorganized and displaced on the left side.
 Figures 4 and 5 |
In the most superior section, the neoplasm was not found around the rectal wall (Fig. 6, 7).
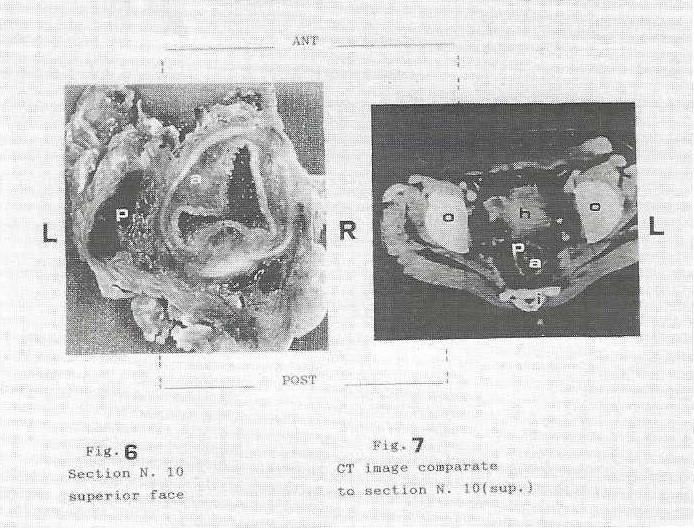 Figures 6 and 7 |
| A: Rectum B: Vagina C: Neoplasm D: Annulus |
E: Pubic Symphysis F: Peritoneum G: Bladder H: Uterus |
I: Sacrum L: Femur M: Rectum Muscle N: Coccygeus |
O: os coxae P: Perirectal vessels |
By comparing CT images and photographs of the macroscopic sections, it was possible to verify the accuracy of the in-vivo instrumental study. It was also possible to explain details ambiguously shown by CT. Thus, plastination can be a useful tool for verifying sophisticated clinical and instrumental images.
Bickley HC: Preservation of gross tissue specimens by plastination. Bull PatholEduc 6:16-22, 1990.
Lane A: Sectional anatomy: standardized method- ology, J. Int. Soc. Plastination, 4:16-22, 1990.
https://doi.org/10.56507/LYMW2924
von Hagens G: Impregnation of soft biological specimens with thermosetting resins and elastomers. Anat. Rec. 194:247-256, 1979. https://doi.org/10.1002/ar.1091940206
von Hagens G: Heidelberg Plastination Folder: Collection of all technical leaflets for plastination. English ed. Anastomoses Institute 1, University Heidelberg, 1985.
von Hagens G.; Klaus, Tiedeman; and Wilhelm Kriz: The current potential of plastination. Anatomy and Embryology 175: 411-21, 1987. https://doi.org/10.1007/BF00309677