1 Department of Anatomy, Histology and Embryology, Faculty of Medicine, University of Debrecen, Debrecen, Hungary
2 Department of Forensic Medicine, Faculty of Medicine, University of Debrecen, Debrecen, Hungary
#Contributed equally to this work
This study presents the dissection of a lower limb from a deceased individual who underwent reconstructive surgery due to a right tibial fracture affecting both the medial and lateral condyles of the proximal epiphysis (plateau fracture). The fracture was corrected using an open reduction internal fixation (ORIF) procedure, where stainless steel plates and screws were implanted. During the dissection in the area distal to the region affected by the surgery, inappropriate fixation was identified, which resulted in fragile structures that were challenging to dissect and preserve. The dissection was carried out using basic anatomical dissection instruments and the entire process has been documented with photographs in a step-by-step manner. The exposure of the surgical area involved removing the connective tissue covering the implanted hardware, revealing their positioning. Challenges arose in preserving structures located in the insufficiently fixed area, as their fragility limited complete visibility. Following the dissection, the specimen was plastinated and preserved for future educational purposes.
Despite these difficulties, the meticulous dissection and subsequent plastination of the limb yielded a durable specimen that serves educational purposes. This specimen allows demonstration of pathological changes in the tissue, provides a learning experience for surgeons and contributes to a deeper understanding of the healing process that takes place in the postoperative period after traumatological or orthopaedic interventions.
plastination; orthopaedics; surgery; tibial fractures; epiphyses; postoperative period
Tamás Juhász1, Department of Anatomy, Histology and Embryology, University of Debrecen, Faculty of Medicine, Nagyerdei krt. 98, H-4032, Debrecen, Hungary. Tel.: +36-52-255-567; fax: +36-52-255-115.
Email: juhaszt@anat.med.unideb.hu

![]()



Understanding lower limb anatomy is essential for medical and health science students, especially those aspiring to become orthopaedic surgeons or traumatologists. To deepen their knowledge, students may dissect cadavers or use online resources. Education typically starts with basic terminology and limb orientation, progresses to surface landmarks and then explores deeper gross structures (Estai & Bunt, 2016). Dissection labs provide hands-on experience, mainly on formalin-fixed cadavers (So et al., 2017; Roxburgh & Evans, 2021). Medical imaging such as ultrasound, MRI and CT scans supplement traditional learning, while case studies enhance understanding of clinical correlations and pathologies (So et al., 2017; Pettersson et al., 2023). Clinical skills sessions often involve examining patients' lower limbs, emphasizing the importance of understanding anatomical variations for managing complications (Qazi et al., 2022). Pathology discussions, like fractures and dislocations, highlight clinical relevance, though real post-traumatic cases are rarely seen in dissecting labs (Nicola & Jewison, 2012). Learning common traumatological procedures is vital for future healthcare providers. During classes, students study the physiological positions of structures, traumatic injuries and treatment options, but postoperative conditions are seldom addressed in gross dissections, as these tissues are not preserved long-term (Dykyj & Jules, 1991). Understanding lower limb biomechanics post-surgery is crucial for physiotherapy (Esquenazi, 2014). Workshops on surgical anatomy prepare students for specialties but often do not focus on healing or postoperative complications. Integrating anatomy and pathology in postoperative education offers a more comprehensive understanding of patient recovery. Emerging technologies like plastination are increasingly used to preserve rare or postoperative cases, enhancing traumatological training (Kukulski et al., 2023).
While plastination of healed fractures remains challenging, the classification of fractures, such as bicondylar tibia fractures, is well-studied. Accurate treatment depends on proper categorization, with the Müller-AO classification being most common (Nguyen et al., 2020b; Besa et al., 2023). Soft tissue conditions, classified by systems like Gustillo-Anderson, also influence treatment outcomes (Plotnikovs et al., 2022). Fractures in the crural region are complex due to the tibia's load-bearing role and soft tissue coverage, requiring advanced imaging (CT, MRI, angiography) for planning. Treatment varies from conservative methods, such as casting and external fixation, to surgical interventions such as osteosynthesis with plates or intramedullary nailing (Nguyen et al., 2020a; Du et al., 2021). Traditional plates, once common, now see limited use due to infection risks and the rise of intramedullary nailing and angular stable plates. These interventions are typically studied during residency or workshops, but postoperative healing is rarely examined in anatomical or traumatological education, with follow-up imaging confirming implant positioning but not explored during dissections.
In this study, a lower limb was dissected post-surgery. Healing in a not well-fixed area was examined and preserved via plastination for educational purposes. Dissection also revealed stainless steel plates in the postoperative period, which were maintained in their position after plastination. The focus was on preserving and studying postoperative conditions of surgical intervention.
The donation of the body for anatomical examination took place according to the binding legal regulations. The cadaver was fixed with 10% formalin via the femoral artery at 1.2 bar pressure, and formalin was circulated in the body to reach the tissues. The cadaver was then placed into a 10 % formalin bath for 3 months. The preservation process was performed in accordance with the routine protocol of the Department of Anatomy, Histology and Embryology at the University of Debrecen, Hungary. After preservation, the lower limbs connected to the pelvis were separated at the level of the iliac crest, and the pelvis was halved in the sagittal plane. Dissection involved basic scalpels, scissors and forceps. Scar tissue covering the implanted plates and screws was removed with surgical scalpels. A Pean clamp was used to retract muscles and tendons.
An anatomical dissection of a complete lower limb from a deceased individual who had surgical intervention for a tibial fracture was conducted for educational purposes. The detailed medical history was unknown, but we were informed that the deceased had undergone knee surgery. The exact type of intervention was determined after exposing the surgical area. The deceased likely suffered a plateau fracture of the medial and lateral tibial condyles, known as a bicondylar tibial plateau fracture. The fracture had been corrected with open reduction and internal fixation (ORIF), during which two buttress steel plates and several screws were implanted.
After dissection, the specimen was dehydrated by immersion in acetone at -20° C for approximately 3 weeks. Then the specimen was placed in a vacuum chamber (at atmospheric pressure) with liquid silicone (S10/S3 BIODUR® Products GmbH, Heidelberg, Germany) until vacuum removed the remaining air, allowing the silicone to infiltrate the specimen. This step took approximately 4 weeks in the case of the complete lower limb. After impregnation, the specimen was kept at room temperature in a chamber for 7 days while excess silicone drained from the tissues. Silicone droplets were removed and the surface of the specimen was wiped every day. During this process, anatomical structures were positioned and separated for the best possible visualization of obscured structures. For the final step, the dissected specimen was placed in the S6 (BIODUR® Products GmbH, Heidelberg, Germany) gas chamber for curing for 10 days at room temperature. The curing process hardened the silicone and ensured that the specimen was stable and retained its shape. The curing process preserved the status of degraded tissues as well.
Anatomical dissection revealed a lower limb with bicondylar tibial plateau fracture treated via ORIF with steel plates and screws, following prior knee surgery. Unfortunately, such interventions can lead to numerous complications despite the greatest precautions. Complications such as infection, swelling, bone damage, secondary displacement of the fracture and acute compartment syndrome may occur (Rudran et al., 2020; Amin et al., 2021; Milenkovic et al., 2021). In severe cases, the implanted hardware can cause inflammation, vascular occlusion and knee arthrofibrosis (Choo & Morshed, 2014; Kugelman et al., 2017).
During the dissection of the lower limb, our primary goal was to expose the surgical area in such a way as to preserve the important anatomical structures while ensuring that the implanted screws and plates were clearly visible to demonstrate features of the healing process. Finally, our objective was to prepare the specimen for plastination so that it could be used for educational purposes for a longer duration.

Figure 1 -Location of screws on the anteromedial surface of the tibia. (A) Position of flexible plates and screws; (B) protrusion of screws from the bone surface. Red circles highlight the elevation of stainless steel screws. Arrows 1 and 3: flexible plate and surrounding healing tissue; arrow 2 indicates anatomical position of tibia
The dissection proceeded normally for the regions above the knee, and we successfully preserved all significant anatomical structures. During the exposure of the knee region, we found several screws and two buttress steel plates on either side of the proximal epiphysis of the tibia (Fig. 1A). Among the placed hardware, we found several screws that protruded significantly 7 mm above the plane of the plate (Fig. 1B). In the case of one screw, it was observed that the tip of the screw significantly exceeded the bony substance (Fig. 1B). While this is an expected consequence of the healing process (Amin et al., 2021) the extent of the protrusion of the screw was surprising. Moreover, the tip of one screw was positioned towards the popliteal artery and vein, although the surrounding tissue was well dissectible in this area (Fig. 2).
During dissection of the distal (crural and plantar) regions, tissues below the knee were fragile, likely due to transient acute compartment syndrome (Cleveland Clinic, 2024) or circulatory issues from popliteal artery compression (Fig. 3A). This limited our ability to fully dissect deeper vascular and nerve structures; the anterior tibial and fibular (peroneal) muscles were partially disintegrated, and the superficial fibular (peroneal) nerve was difficult to isolate (Figs. 3A, 3B). The plantar surface posed additional challenges: poor formalin fixation led to inadequate preservation, causing muscle tissue damage during dissection (Fig. 4A). In contrast, the opposite limb's sole was well-preserved (Fig. 4B), supporting the circulatory insufficiency theory, as formalin hadn't penetrated deeper layers. Despite this, vascular and nerve structures remained intact, though superficial plantar muscles were severely damaged. We did not dissect the popliteal artery or its branches to identify the cause of obliteration, prioritizing preservation of anatomical structures.
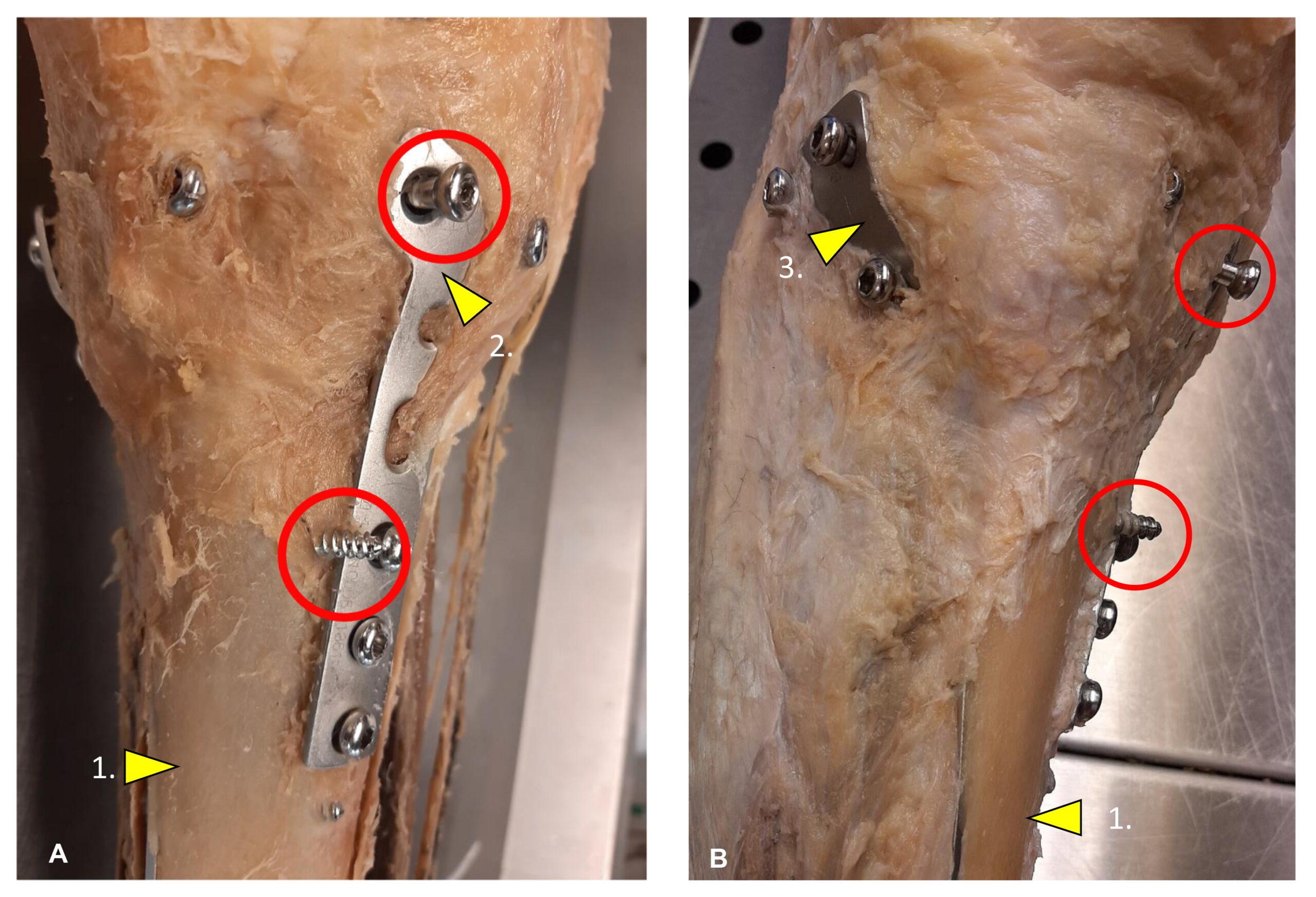 Figure 2 - Screws facing towards popliteal fossa. Dissection of popliteal fossa was normal although the tip of one screw (red circle) pointed to the deep part of the region. Arrowheads: 1, common fibular (peroneal) nerve; 2, tibial nerve; 3, biceps femoris; 4, gastrocnemius |
 Figure 3 - Injury in the anterior crural region. (A) Anterior tibial muscle disintegration and superficial peroneal (fibular) nerve damage; (B). Tissue degradation resulted in muscle and tissue fragility. Arrowheads: 1, disintegration of anterior tibialis muscle; 2, degradation of superficial peroneal (fibular) nerve |
 Figure 4 -Disintegrated tissues in the foot. (A) Plantar region damage in the operated lower limb. Arrowheads: 1, plantar aponeurosis; 2, flexor digitorum brevis; 3, lateral plantar nerve and vessels; 4, medial plantar nerve. |
After dissection, we proceeded with limb plastination. We documented the knee before (Fig. 5A) and after plastination (Fig. 5B). The specimen's volume reduction was notable due to high fluid content in inadequately fixed areas, but this did not affect the macroscopic structures or hardware placement. Plastination preserved fragile regions and clearly displayed the hardware's position relative to the knee. Similarly, the entire limb was documented before (Fig. 6A) and after plastination (Fig. 6B), with all dissected and challenging areas well preserved. The postoperative surgical site remained unchanged throughout the process.
 Figure 5 - The surgical area before and after plastination. (A) Completed anatomical preparation around the surgical area. (B) surgical area after plastination. Plastination preserved the postoperative situation in knee joint without any serious modification. |
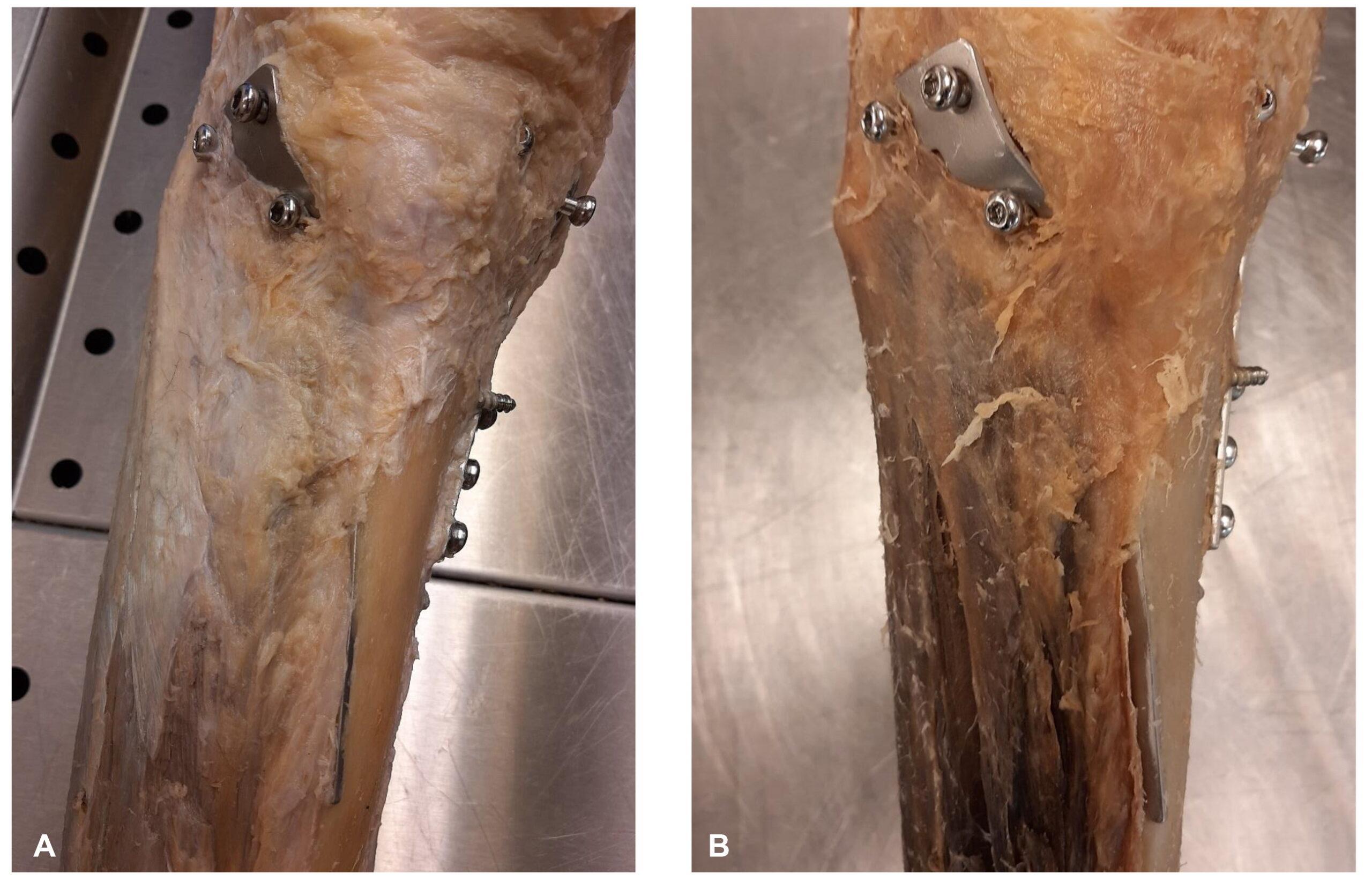 Figure 6 - The dissected lower limb before (A) and after (B) plastination. Completed anatomical preparation of the entire lower limb showing normal shrinkage after plastination |
The crural region consists of two long bones, the tibia and fibula. The tibia is more load-bearing, being one of the strongest yet most frequently fractured bones in the lower limb (Muller et al., 2023). Its anteromedial surface is subcutaneous, making it vulnerable to fractures and open injuries from direct impacts (Ramponi & McSwigan, 2018). In traumatology, orthopaedic surgery, and other medical fields, a detailed understanding of lower limb anatomy is essential. Many anatomical atlases and online resources provide theoretical knowledge, but their idealized representations are less applicable practically. Therefore, specimens preserved via formalin or plastination are valuable for hands-on learning. While some articles focus on pathological cases for education (Goh et al., 2024), most address internal organ deviations like cerebral infarctions, cardiac tamponade, or neoplasms (Alpar et al., 2005). Fewer studies cover limb pathologies, mainly joint abnormalities and vascular visualization (Graf et al., 1991). Publications on limb trauma or surgical abnormalities are scarce, indicating that pathological limb changes and their preservation are only sporadically documented.
Our plastinated lower limb specimen offers an excellent demonstration of a significant surgical intervention for students. Careful dissection aimed to keep the surgical area visible while maintaining surrounding anatomical relationships. Preserving degraded tissues below the knee was challenging, extending dissection time, but plastination preserved these regions well, enhancing specimen longevity. However, plastination reduces water content (Monteiro et al., 2022), which may influence postoperative condition assessments. Nonetheless, it does not hinder topographical analysis of implants used in trauma surgery and allows study of tissue degradation.
For medical education, it is vital for students and residents to understand both normal anatomy and changes during postoperative recovery. This specimen facilitates study of external fixation, osteosynthesis plates and intramedullary nailing. Although some efforts exist to present pathological or postoperative changes (Simank et al., 1997), such studies are limited, especially regarding post-surgical limb alterations. Despite advances in imaging and 3D printing for surgical planning, understanding degenerative postoperative processes remains challenging (Chen et al., 2024). This plastinated specimen provides valuable insights for students to master anatomy and to discuss pathological conditions such as fractures and healing processes. Such dissections deepen anatomical knowledge, broaden clinical perspectives and support future studies in various specialties.
Acknowledgements
The authors are grateful to Péter Ágoston, Sándor Fodor and Balázs Gibárti for excellent technical assistance. The authors sincerely thank those who donated their bodies to science so that anatomical research could be performed. Results from such research can potentially increase mankind’s overall knowledge, which can then improve patient care. The research was supported by NKFIHK139396
Ethical Approval
This study was performed in line with the principles of the Declaration of Helsinki. Cadaver donation for anatomical dissection happened according to the binding legal regulations of the University of Debrecen.
Alpar A, Glasz T, and Kalman M. 2005: Plastination of pathological specimens - A continuing challenge. J Int Soc Plastination 20: 8-12. https://doi.org/10.56507/TFCD4856
Amin TK, Patel I, Patel MJ, Kazi MM, Kachhad K and Modi DR. 2021: Evaluation of results of open reduction and internal fixation (ORIF) of fracture of distal end of femur with intra-articular extension. Malays Orthop J 15: 78-83. https://doi.org/10.5704/MOJ.2111.012
Besa P, Angulo M, Vial R, Vega R, Irribarra L, Lobos D, Sandoval F and Irarrazaval S. 2023: The AO classification system for tibial plateau fractures: An independent inter and intraobserver agreement study. Injury 54 (Suppl 6): 110741. https://doi.org/10.1016/j.injury.2023.04.028
Chen T, Chen J, Li X, He Y, Peng Q and Chen H. 2024: A comparative study on 3D printing-assisted arthroscopic IDEAL point femoral tunnel positioning for anterior cruciate ligament reconstruction versus conventional arthroscopic positioning. BMC Musculoskelet Disord 25: 481. https://doi.org/10.1186/s12891-024-07591-y
Choo KJ and Morshed S. 2014: Postoperative complications after repair of tibial plateau fractures. J Knee Surg 27: 11-19. https://doi.org/10.1055/s-0033-1363517
Cleveland Clinic 2024: Open reduction and internal fixation (ORIF). URL: https://my.clevelandclinic.org/health/procedures/open-reduction-and-internal-fixation-orif
Du S, Wei L, He B, Fang Z, Zhou E, Ma X and Li J. 2021: Dynamic fixation using rigid tape in rehabilitation after surgery of terrible triad injury of the elbow: A randomized trial. J Back Musculoskelet Rehabil 34: 957-964.
https://doi.org/10.3233/BMR-200279
Dykyj D and Jules KT. 1991: The clinical anatomy of tendons. J Am Podiatr Med Assoc 81: 358-365.
https://doi.org/10.7547/87507315-81-7-358
Esquenazi A. 2014: Gait analysis in lower-limb amputation and prosthetic rehabilitation. Phys Med Rehabil Clin N Am 25: 153-167. https://doi.org/10.1016/j.pmr.2013.09.006
Estai M and Bunt S. 2016: Best teaching practices in anatomy education: A critical review. Ann Anat 208: 151-157. https://doi.org/10.1016/j.aanat.2016.02.010
Goh JSK, Chandrasekaran R, Sirasanagandla SR, Acharyya S and Mogali SR. 2024: Efficacy of plastinated specimens in anatomy education: A systematic review and meta-analysis. Anat Sci Educ 17: 712-721.
https://doi.org/10.1002/ase.2424
Graf J, Fromm B, Schneider U and Niethard FU. 1991: The application of the plastination method in experimental orthopaedic surgery. J Int Soc Plastination 5(1): 20-22. https://doi.org/10.56507/RBNR4372
Kugelman D, Qatu A, Haglin J, Leucht P, Konda S and Egol K. 2017: Complications and unplanned outcomes following operative treatment of tibial plateau fractures. Injury 48: 2221-2229.
https://doi.org/10.1016/j.injury.2017.07.016
Kukulski J, Rausa J, Weld J, Jaji A, Ikeda N, Lee B, Thomas L, Anderson RH and Loomba RS. 2023: The utility of a structured, interactive cardiac anatomy teaching session for resident education. Cardiol Young 33: 208-212.
https://doi.org/10.1017/S1047951122000440
Lin KC, Huang FT, Chen CY and Tarng YW. 2024: Is staged surgery always necessary for Schatzker type IV-VI tibial plateau fractures? A comparison study. Life (Basel) 14(6): 753 https://doi.org/10.3390/life14060753
Milenkovic S, Mitkovic M, Mitkovic M, Stojiljkovic P and Stojanovic M. 2021: Lateral tibial plateau fractures - functional outcomes and complications after open reduction and internal fixation. Int Orthop 45: 1071-1076.
https://doi.org/10.1007/s00264-020-04763-y
Monteiro YF, Silva MVF, Bittencourt A and Bittencourt AS. 2022: Plastination with low viscosity silicone: strategy for less tissue shrinkage. Braz J Med Biol Res 55: e11962. https://doi.org/10.1590/1414-431x2022e11962
Muller M, Kahl U, Von Roth P and Hube R. 2023: Intraoperative fractures of the tibia and femur in knee revision surgery. Z Orthop Unfall 161: 85-91. https://doi.org/10.1055/a-1542-9192
Nguyen TN, Carpanen D, Rankin IA, Ramasamy A, Breeze J, Proud WG, Clasper JC and Masouros SD. 2020a: Mapping the risk of fracture of the tibia from penetrating fragments. Front Bioeng Biotechnol 8: 544214.
https://doi.org/10.3389/fbioe.2020.544214
Nguyen TN, Carpanen D, Stinner D, Rankin IA, Ramasamy A, Breeze J, Proud WG, Clasper JC and Masouros SD. 2020b:. The risk of fracture to the tibia from a fragment simulating projectile. J Mech Behav Biomed Mater 102: 103525. https://doi.org/10.1016/j.jmbbm.2019.103525
Nicola TL and Jewison, DJ. 2012: The anatomy and biomechanics of running. Clin Sports Med 31: 187-201.
https://doi.org/10.1016/j.csm.2011.10.001
Pettersson AF, Karlgren K, Al-Saadi J, Hjelmqvist H, Meister B, Zeberg H and Silen C. 2023: How students discern anatomical structures using digital three-dimensional visualizations in anatomy education. Anat Sci Educ 16: 452-464. https://doi.org/10.1002/ase.2255
Plotnikovs K, Ribakovs O, Movcans J, Pasters V and Solomin LN. 2022: A 52-year-old man with a Gustillo-Anderson IIIB open tibial shaft fracture with extensive soft-tissue defect requiring limb salvage with artificial deformity-creating technique. Am J Case Rep 23: e934788. https://doi.org/10.12659/AJCR.934788
Qazi E, Wilting J, Patel NR, Alenezi AO, Kennedy SA, Tan KT, Jaberi, A and Mafeld S. 2022: Arteries of the lower limb - embryology, variations, and clinical significance. Can Assoc Radiol J 73: 259-270.
https://doi.org/10.1177/08465371211003860
Ramponi DR and Mcswigan T. 2018: Tibial plateau fractures. Adv Emerg Nurs J 40: 155-161.
https://doi.org/10.1097/TME.0000000000000194
Roxburgh M and Evans DJR. 2021: Assessing anatomy education: A perspective from design. Anat Sci Educ 14, 277-286. https://doi.org/10.1002/ase.2060
Rudran B, Little C, Wiik A and Logishetty K. 2020: Tibial plateau fracture: Anatomy, diagnosis and management. Br J Hosp Med (Lond) 81: 1-9. https://doi.org/10.12968/hmed.2020.0339
Simank HG, Graf J, Kerber A and Wiedmaier S. 1997: Long-term effects of core decompression by drilling. Demonstration of bone healing and vessel ingrowth in an animal study. Acta Anat (Basel) 158: 185-191.
https://doi.org/10.1159/000147929
So S, Patel RM and Orebaugh SL. 2017: Ultrasound imaging in medical student education: Impact on learning anatomy and physical diagnosis. Anat Sci Educ 10: 176-189. https://doi.org/10.1002/ase.1630