Division of Anatomical Sciences, Office of Medical Education, The University of Michigan Medical School, Ann Arbor, Michigan, 48109-0608, USA.
Medical students studying human gross anatomy often have difficulty conceptualizing the internal three-dimensional structure of organs and the pattern of distribution of blood vessels. Students are further challenged with comprehending the orientation and spatial relationship different organs have to one another as they function as integral parts of systems. Although tracheobronchial and heart casts of animals have been produced and have proven to be valuable tools in veterinary medical education (Henry, et al., 1992, 1998), few efforts have been made to develop physical models of these internal structures in humans for use in medical education. In this work, colored silicone casts of a human heart, tracheobronchial tree, and brain ventricles were made from unembalmed organs. Major vessels were cannulated, and appropriately colored silicone was injected. Specimens were macerated to yield resilient, anatomically exact replica of the internal architecture such as cardiac chambers, lung vessels and airways, and the brain ventricular system.
cast; silicone; tracheobronchial; ventricles
A. RAOOF: Office of Medical Education, The University of Michigan Medical School, 3808 Med. Sci. IIBldg., Ann Arbor, Ml, 48109-0608, USA; Telephone: 734-615 2597; Fax: 734-615 8191; E-mail: ameedr@umich.edu

![]()



Research has indicated that engaging multiple senses enhances learning in academic settings. (Kundall, 1990; Westman, 1990). One of the challenges facing medical educators is presenting the circulatory and respiratory systems of humans, namely the heart and the lungs; in such a way that conceptualization of their spatial interaction and interdependence is achieved. Visualizing pulmonary and systemic circulations through the chambers and great vessels of the heart and the pulmonary vessels of the lungs, and relating these to the tracheobronchial tree, is difficult for medical students to understand using two-dimensional illustrations, dissections, videos and computer simulations.
Color-coded casts of the heart/lung system have proven invaluable for teaching medical gross anatomy. By acquiring greater understanding of the spatial relationship of overlapping circulatory vessels and the lobes of the lungs, for instance, students are better equipped to efficiently and accurately examine patients and to interpret diagnostic images of the thoracic cavity. The anatomical accuracy and durability of casts make them powerful tools to accelerate knowledge acquisition and strengthens diagnostic abilities for medical students utilizing a wider variety of learning strategies.
The tracheobronchial, heart, and brain casting techniques used in this work were based on those of Tompsett (1970); Henry et al. (1992, 1998); and Grondin et al. (2000).
Preparation:
The heart, lungs, and brain were freshly harvested from human cadavers donated to the University of Michigan Anatomical Donation Program. Initially, all vessels and passageways of each organ were thoroughly rinsed with warm water to remove residual blood clots. Specimens were placed in a running water bath overnight before injection commenced the following day. If injection was planned for a later time, 3-5% formaldehyde was added. Water remaining in the vessels was flushed out using compressed air before injection.
Brain specimens were kept in 5% formaldehyde solution for about 3-5 days to ensure sufficient firmness during handling.
Three lungs and 2 heart-lung specimens as well as two brains were used in this work. All rubber cannulas used for injecting silicone were made of clear vinyl tubing of _ inch inner diameter fitted with a steel screw- type syringe adapter on one end.
Heart-lung specimen: Both lungs and heart were kept connected to each other. The pericardium was removed and the inferior vena cava was clamped with a hemostat. A 15 inch long cannula was pushed into the superior vena cava, through the tricuspid valve to the right ventricle, and into the pulmonary conus. A short incision, approximately an inch in length, was made in the ascending aorta and a second similar cannula was inserted into the left ventricle and then pushed through the mitral valve into the left atrium. This procedure ensured that the silicone would fill up the pulmonary veins. Cannulas were firmly retained in place with a piece of waxed string.
Lung specimen: The pulmonary artery and vein were cannulated. A third cannula was inserted and bound in the trachea for subsequent injection of the airways of the lungs. Cannulas used here were 10 inches in length. (Fig. 1).
Brain: A one inch diameter opening was drilled at the top of each cerebral hemisphere at the site of the central sulcus using an ordinary brass cork borer to provide access to the lateral ventricles. The ventricles were flushed with water and a 6 inch cannula was gently inserted into one opening (Fig. 2).
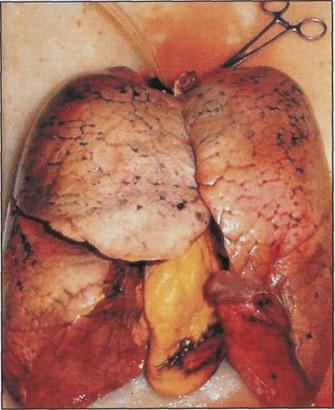 Figure 1. Preparation of a lung-heart specimen for silicone injection. |
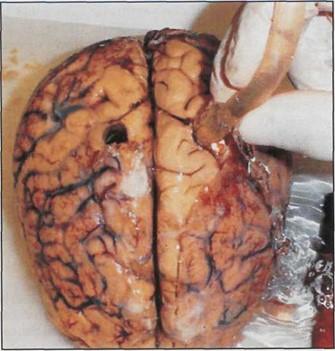 Figure 2. Cannulation of brain specimen before injecting silicone. |
Silicone injection:
The specimens were injected with E RTV Silicone (Dow Corning, Midland, MI, USA) at room temperature. The silicone was colored red and blue with Biodur E20 (Biodur, Heidelberg, Germany) until the desired color shade was achieved. RTV Silicone Rubber Curing Agent was added at a 1:10 ratio to the silicone polymer immediately prior to injection. Injection was achieved using 60ml syringes filled with 35ml aliquots. The viscosity of the silicone was high enough to necessitate the use of a caulk gun to force the compound through the syringe into the cannula. Filling the syringe to 35ml extended the length of the syringe so that it was able to fit into the caulk gun. In the lungs, injection was stopped when silicone was visible under the surface of both lungs. In the heart-lung specimen, cannulas were pulled out slowly and gradually while injection was still maintained to ensure that silicone would fill the atria and ventricles. Silicone was kept from oozing out by using hemostats and waxed strings whenever necessary. In the brain, silicone was gently pushed into one cannula and injection was stopped when silicone started emerging through the opening on the next hemisphere.
Curing:
Following injection, the silicone was allowed 24-48 hours at room temperature to harden before maceration.
Maceration:
After the silicone hardened, specimens were placed in a freshly prepared 10% potassium hydroxide (Potassium Hydroxide Flakes, Fisher scientific, USA) solution for 5-7 days and then left in boiling water for 8-12 hours to detach tissues from the polymer. Following maceration in boiling water, the specimens were placed in 5% hydrogen peroxide for about 2 hours to complete the removal of residual tissues. Casts were then rinsed in running water overnight.
The casts of tracheobronchial tree, heart chambers, and brain ventricles were of excellent quality in terms of flexibility, clarity of details, and anatomical accuracy. The tracheobronchial and vascular tree casts showed clear color distinction that was clear throughout the minor bronchioles and vascular branching (Figs. 3, 4). Brain ventricular casts showed lateral ventricles, the third and most of the fourth ventricles with almost complete filling (Fig. 5).
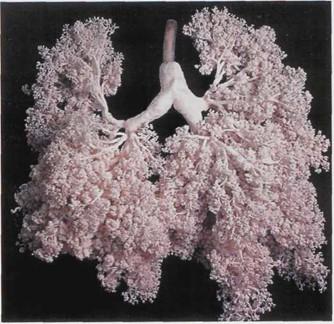 Figure 3. Tracheobronchial silicone cast. |
 Figure 4. Tracheobronchial and heart cast using colored silicone. |
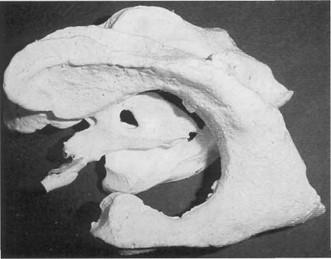 Figure 5. Brain ventricular cast. |
Silicone injection through vessels was relatively effortless when the concentration of formaldehyde during preparation stage was 5% or less. Higher concentrations of formaldehyde made vessels firmer and hence injection was difficult. Also, we found that the degree of silicone flow through vessels and ventricles as well as the time needed for complete hardening following the injection were directly related to the concentration of the RTV Silicone Rubber Curing agent where 10% gave optimal results. Regarding maceration, better results were produced using fresh 10% potassium hydroxide for 5-7 days followed by boiling. Higher concentrations of potassium hydroxide or longer immersion of organs resulted in digestion of the silicone casts and loss of vascular fine details.
Silicone casts of vessels, tracheobronchial tree, and brain produced in our lab were sturdy and anatomically precise. Specimens' sturdiness was generally assessed in terms of flexibility during regular handling and stretching. Used to enhance medical student learning in gross anatomy, these casts provide precise visual representations of the difficult to perceive internal architecture of these organs. Consequently, knowledge acquisition by students may occur faster as they employ multiple senses to both see and feel actual representations of each organ. Coupled with the use of silicone-plastinated hearts and lungs conceptualization of difficult physiological processes within these organs is made easier. Students' knowledge, clinical examination and diagnostic skills, accordingly, are enriched. During gross anatomy lab sessions at our medical school, medical students attended the course often used these casts in understanding the complex patterns of the tracheobronchial tree and the brain ventricular system. A formal study based on a thorough questionnaire to assess the usefulness of these casts in medical education is under preparation.
Some challenges for production of silicone casts of specimens arising from human cadavers, however, should be noted. At the University of Michigan, over 90% of anatomical donations are from elderly patients. Hence, a variety of clinical conditions may be encountered that impede quick and efficient production of silicone casts. In one specific case, a donor whose heart and lungs were slated for casting suffered a cardiac tamponade resulting from a ruptured aorta. Though the ruptured aorta was surely the cause of death, apparent pneumonia developed in the right lung before death and severely diminished the integrity of the lung. As a result, the lung was rendered useless for casting purposes due to deterioration of most of the tracheobronchial pathways. Some damage also occurred to the lung tissue during harvesting due to extensive adhesions to the thoracic wall.
In another incident, red-colored silicone injected into the pulmonary vein in an attempt to fill the left atrium and ventricle of another donor, had filled the entire heart instead. One possibility for this occurrence was that the donor suffered from a congenital septal defect that became apparent during the casting process.
Collapsed lungs, breast cancer metastasis into internal organs, and excessive accumulations of fat in and around organs of interest are further medical phenomena that can encumber the casting process. While human anatomical donations given to further the pursuit of medical knowledge, full-scale production of accurate, detailed casts must respectfully yield to the weakened state of some donors' organs, many which arise from older individuals. However, castings of pathological specimens may in time provide a valuable tool of comparison between normal and pathological specimens. Also, we are working on casting other organs like the liver and vascular casts of brain and kidneys.
The quality of the brain ventricular casts could be enhanced by ensuring a complete filling of all ventricles. This issue is currently under investigation taking into account the technique applied by Grondin et al. (2000).
An air pressurized injection method is being developed to add speed and efficiency to the casting process. As it is, the injection process is sometimes slow and laborious. With the increasing demand for the specimens and number of students handling these specimens, there is a need to accelerate the injection process. The air-pressurized method, utilizing the compressed air available at the lab, will allow us to quickly inject a number of specimens. It will also allow a more controlled flow of silicone with the use of pressure gauges and shut-off valves. With these two factors, we plan to create a plentiful stock of higher quality casts.
It is hoped that organ casting will make a significant contribution to medical education being an affordable and easy technique for visualizing anatomical specimens.
Grondin, J., Sianothai, A., Olry, R. 2000: In situ ventricular casts of S10 plastinated human brains. J Int Soc Plastination 15(1):18-21.
https://doi.org/10.56507/APKG6089
Henry RW, Daniel, GB, Reed, RB. 1998: Silicone Castings of the Chambers of the Heart and the Great Vessels. J Int Soc Plastination 13(1):17-19.
https://doi.org/10.56507/AWGT3303
Henry, RW. 1998: Silicone Tracheobronchial Casts. J Int Soc Plastination 6:38-40.
https://doi.org/10.56507/LOVB7516
Kundel, HL. 1990: Visual clues in the Interpretation of Medical Images. J Clin Neurophysiology 7(4):472-
https://doi.org/10.1097/00004691-199010000-00003
Westman, AS. 1990: Picture books, not readers! Teachers use the wrong modality in presentations and students in studying. Percept Mot Skills 70(3, part 1): 840-2.
https://doi.org/10.2466/pms.1990.70.3.840
Oleksik, SA. 1987: Learning through Visualization. Nurse Educator 12(6):36-7.
https://doi.org/10.1097/00006223-198712060-00012
Tompsett, D.H. 1970: Anatomical Techniques. Second edition, E. & S. Livingstone, London.