1Department of Anatomy, Christian Medical College, Vellore, India, The Tamil Nadu Dr. MGR Medical University, Chennai
2Department of Radiotherapy, Christian Medical College, Vellore, India, The Tamil Nadu Dr. MGR Medical University, Chennai
| Recent advances in plastination have shown that lightweight plastination is cost-effective. For radiotherapy treatment planning, an anatomically accurate phantom is of greater use than the commercially available Alderson Rando phantom. The aim of this study is to develop a lightweight plastinated phantom and validate its radiological property for dosimetry in radiotherapy planning. Formalin fixed specimens were plastinated using lightweight plastination technique. CT imaging was done before and after plastination. The CT numbers and volumes of organs were compared. The radiological tissue properties of bone, soft tissue, and lung substitutes of the Alderson Rando phantom were compared with the lightweight plastinated phantom. The plastinated phantom was irradiated as per an IMRT (intensity-modulated radiotherapy treatment) plan consisting of 7 fields for 6 MV x-rays, generated using Eclipse Treatment Planning System (TPS). The measured doses were compared with the calculated doses of TPS. The lightweight plastinated phantom obtained was dry, robust and light. The radiological properties of the lightweight plastinates were closer to the cadaver. The CT numbers and electron density of soft tissue and lungs of the light-weight phantom was comparable to the Alderson Rando phantom. The dose difference between the measured and calculated dose for IMRT for Planning target volume, lung (right), lung (Left), spinal cord and liver were -3.3, +12.3, -0.2, -1.27 and +0.17 cGy respectively. In conclusion, radiological properties of the cost-effective lightweight plastinated phantom are comparable with the Alderson Rando phantom, which suggests that the light-weight plastinated phantoms can be used for dosimetry in radiotherapy. |
CT number; IMRT; Alderson Rando phantom; dosimetry; xylene
Dr Pauline Shanthi, Department of Anatomy, Christian Medical College, Vellore, India 632002
telephone +91 9486887846, pauline.shanthi@cmcvellore.ac.in

![]()



Plastination is a unique technique of tissue preservation where water and lipids in biological tissues are replaced by curable polymers which are subsequently hardened, resulting in dry and durable specimens. Since its invention, research has been done by various authors to improve the quality of the plastinated specimens. One such improvement is the lightweight plastination technique (Steinke et al., 2008) which requires less resin and thus more tissue-equivalent, and is cost-effective.
For radiotherapy treatment planning, a more anatomically accurate phantom could potentially be of greater use. Phantoms are materials that outfit the dosimeter to ensure a controlled environment around the measurement point and are commonly used in medical imaging and radiotherapy for dosimetric validation (Frigo, 2014). In common, commercially obtained phantoms such as Alderson Rando phantoms are used for most of the dosimetric verifications. However, Alderson Rando phantoms are costly and have only bone, lung, and soft tissue substitutes, but no other organs (Alderson et al., 1962).
A novel anthropomorphic lung phantom was developed by plastination of a pig lung. The plastinated phantom was characterized and compared with reference to in vivo images of the same tissue prior to plastination using high resolution 3D CT. The preservation of anatomical features in the plastinated phantom was confirmed using volume estimates (Yoon et al., 2008). In our previous study (Shanthi et al. 2015), a plastinated phantom was developed using the standard S-10 technique, and its radiological properties were studied which showed higher CT numbers when compared to the cadaver. The higher CT number was attributed to the denser resin. In this study, we proposed to use a lightweight plastinated phantom that could suitably replace the commercial anthropomorphic phantom, and validate its radiological properties for dosimetry in radiotherapy planning.
Ethical approval for this study was obtained from the Institutional Review Board of our institution.
Development and imaging of the lightweight plastinated phantom
A formalin-fixed male cadaver trunk was cut into 5-10 cm slices and then CT scan was carried out using a Philips CT Brilliance 6-slice machine. The digital images were stored in the Picture Archival and Communication System (PACS). The sections were then plastinated using the lightweight plastination technique (Steinke et al., 2008). The sections were dehydrated with acetone at -25 °C and then impregnated in a vacuum chamber in a mixture of Biodur® silicone (S-10) and S3 (hardener) in a ratio of 100:1. Xylene was added to this mixture in the ratio of 1:3 to reduce the density of the polymer. The acetone was slowly replaced by the silicone-xylene mixture over a period of 10 to 14 days. The specimens were then hardened using S6 in a gas chamber. CT scans of lightweight plastinated phantom sections were performed, and the images were transferred to the Treatment Planning System (TPS) (EclipseTM, Varian Medical Systems, Palo Alto, USA, Version 13.7).
Comparison of radiological tissue properties of the cadaver with lightweight plastinated phantom
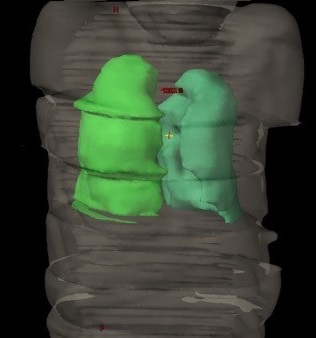 Figure 1. Reconstructed 3D volume of lungs on EclipseTM, Varian Medical Systems, Palo Alto, USA, Version 13.7. |
The radiological tissue properties of liver, spleen, lungs, heart, and body of thoracic vertebra in the sectioned specimens were compared by measuring the CT numbers (in Hounsfield Units) of pre- (cadaveric) and post-plastination specimens, by using TPS. CT numbers were obtained at five different locations within each organ or region of interest, and the average was taken. The volume of organs such as liver, spleen, and lungs, before and after plastination, were measured by contouring the outline of each CT slice from the superior to inferior end of the organ in the TPS. The total extent of the organ contoured was confirmed by the reconstructed 3D volumes created by the TPS, and the percentage shrinkage was then calculated (Fig. 1).
Comparison of the radiological tissue properties of lightweight plastinated phantom with the Alderson Rando phantom
The radiological tissue properties of bone, soft tissue, and lung substitutes of the Alderson Rando phantom were studied by measuring the CT numbers in Hounsfield units, by using the TPS, and compared with that of the bone (vertebra), soft tissue (heart), and lungs of the lightweight plastinated phantom. Relative electron density corresponding to each Hounsfield unit of soft tissue, bone, and lungs was calculated using the formula:
y = 1242.1x - 1054.8
Where ‘y’ is the CT number and ‘x’ is relative electron density.
The attenuation factor was also measured using an optically stimulated luminesce dosimeter (OSLD) in three areas: thorax, abdomen, and pelvis, and compared with TPS values.
Feasibility of using lightweight plastinated phantom in radiotherapy planning
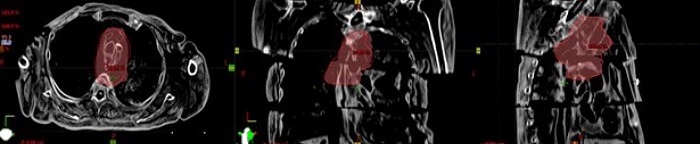 Figure 2. Representation of 95% isodose distribution in axial, coronal, and sagittal views for IMRT plan executed on a lightweight plastinated phantom |
In order to investigate the feasibility of using the lightweight plastinated phantom for clinical dosimetry in radiotherapy, this phantom was used to validate the TPS for intensity-modulated radiation therapy (IMRT). Using the CT images of the lightweight plastinated phantom, an IMRT plan consisting of 7 fields for 6 MV x-rays was generated using Eclipse TPS. The doses were calculated in planning targeted volume (PTV) and the organs at risk (OAR), including right and left lungs, spinal cord, and liver. As well as this, the 95 % isodose distribution around the PTV was also visually assessed as shown in Figure 2. The phantom was then irradiated as per this plan by the linear accelerator, Clinac 2100 CD (Varian Medical System) by placing an optically stimulated luminescence (OSL) dosimeter on the above-mentioned organs in the phantom. The measured doses of these organs were then compared with the calculated dose.
The plastinates obtained were dry, light weighted, and robust (Fig. 3).
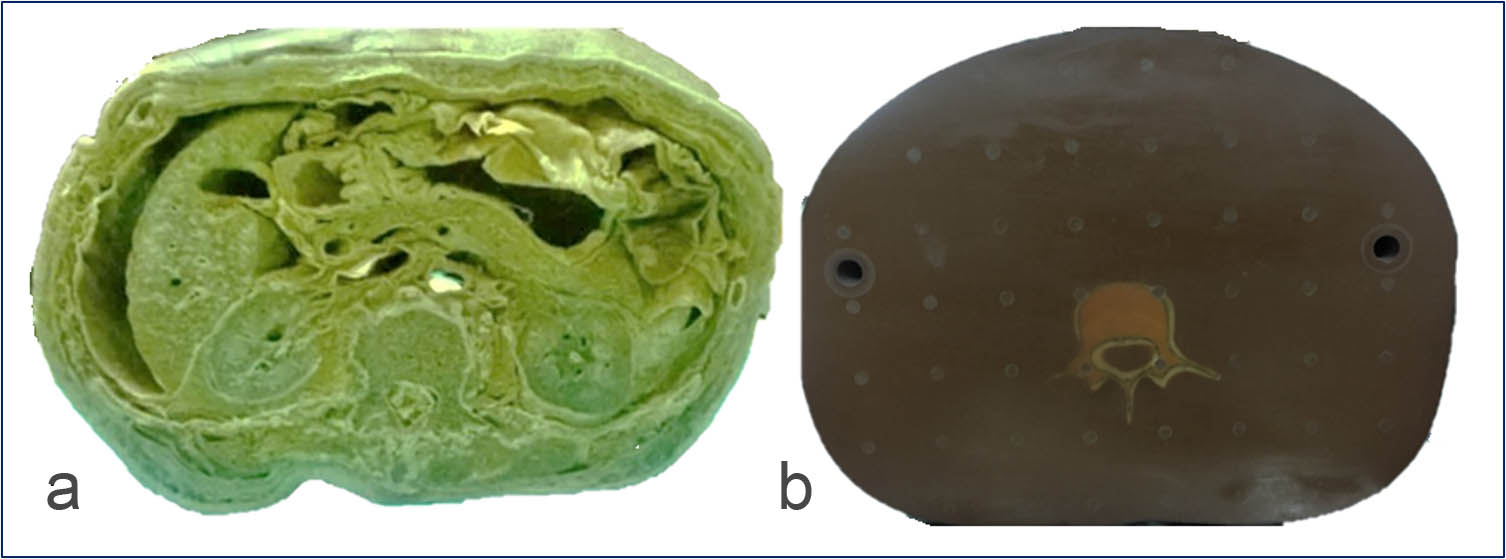 Figure 3. (a) Light weight plastinated phantom showing various organs like lumbar vertebra, kidneys, liver, intestines, blood vessels and muscles; (b) Alderson Rando Phantom showing only bone and tissue substitute. |
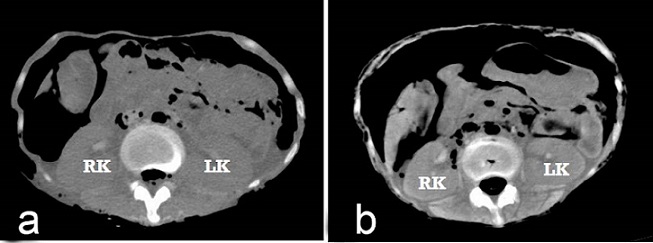 Figure 4. (a) CT image before light-weight plastination (cadaveric); (b) CT image after light-weight plastination (LK-left kidney, RK- right kidney). |
In the CT images of the lightweight plastinated phantom, the fat planes were clear, and organs like lungs, liver, and kidney showed better visual differentiation compared to the pre-plastinated CT images (Fig. 4). On comparing the radiological tissue properties of cadaveric specimens (pre-plastination) with lightweight plastinated phantoms, the CT numbers of the pre- and post-plastination specimens were comparable (Table 1).
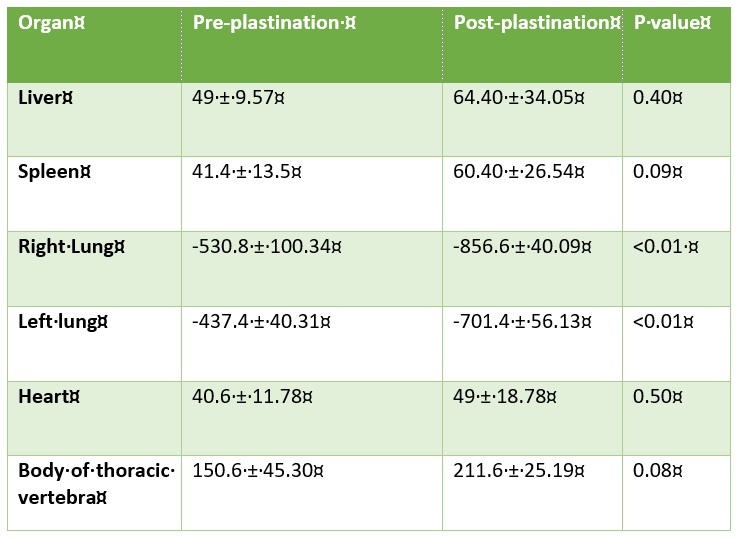 Table 1. CT Numbers of organs in pre-plastinate and post-plastinate in Hounsfield Units. |
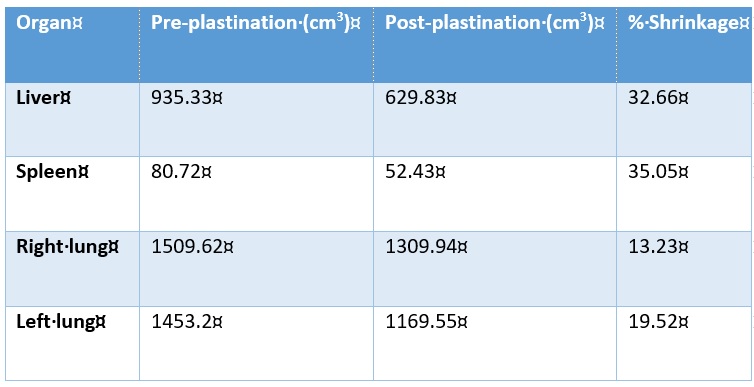 Table 2. Volume estimation of organs before and after light-weight plastination. |
Table 2 shows the volume estimates of the organs before and after lightweight plastination, showing that solid organs had more shrinkage than aerated organs.
Comparison of the radiological tissue properties of lightweight plastinated phantoms with the Alderson Rando phantom
On comparing the radiological tissue properties of lightweight plastinated phantoms with the Alderson Rando phantom and the standard S10 plastinated phantom (Shanthi et al., 2015), the CT numbers and electron density of soft tissue and lungs of the lightweight plastinated phantom were more comparable to the Alderson Rando phantom than those of a standard S10 plastinated phantom (Table 3).
The attenuation values of the lightweight plastinates using the OSL dosimeter were found to be comparable with that of TPS values, with some variation in the ratio values for thorax, abdomen and pelvis, which had a difference of approximately -0.01, -0.01, and -0.02, respectively (Table 4).
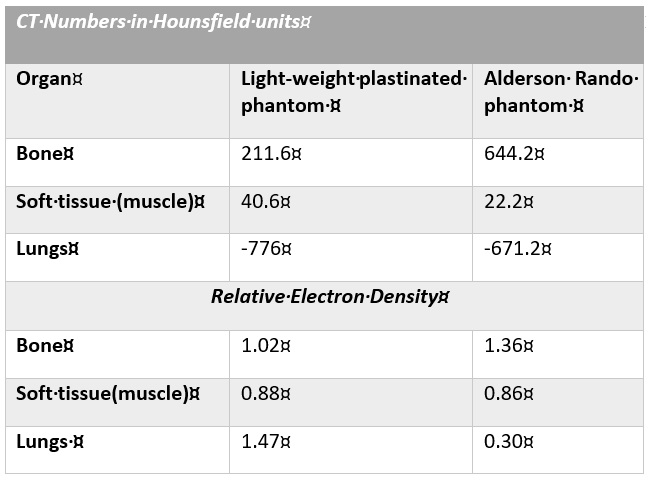 Table 3. Comparison of CT numbers and relative electron density of lightweight plastinated phantom and Alderson Rando phantom. |
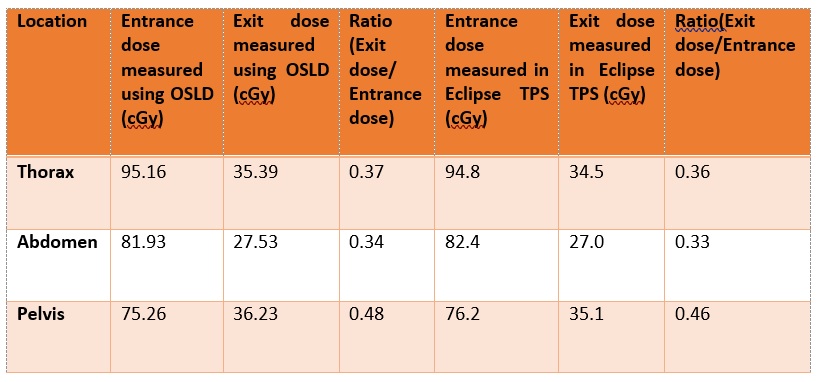 Table 4. Comparison of attenuation factors using OSLD and TPS. |
Validation of TPS using a lightweight plastinated phantom for dosimetry in radiotherapy planning
The measured values of doses using the OSL dosimeter at different locations on the lightweight plastinated phantom with calculated values of doses of the IMRT plan generated with CT images of the lightweight plastinated phantom using TPS, were comparable. The dose difference for PTV, lung (right), lung (Left), spinal cord, and liver was -3.3, +12.3, -0.2, -1.27, and +0.17 cGy, respectively (Table 5). The calculated values of doses of different organs are shown as a dose-volume histogram in Figure 5.
 Figure 5: IMRT plan evaluation using dose volume histogram tool |
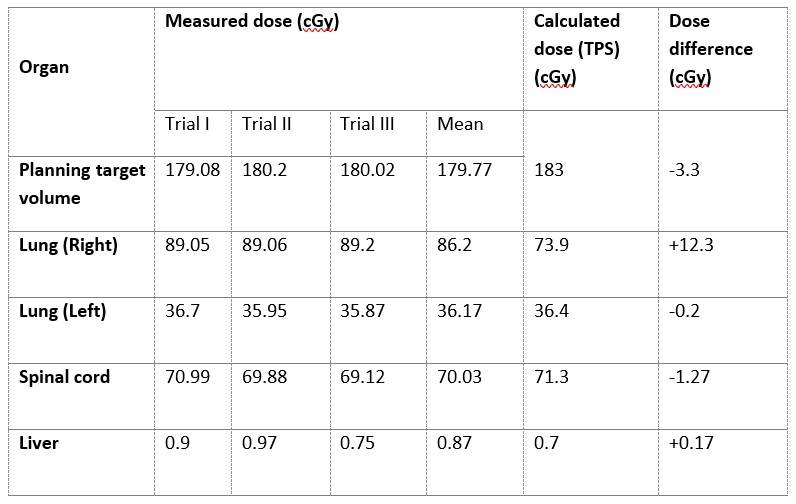 Table 5. Comparison of the measured dose of organ at risk using OSL dosimeter and the calculated dose of the plastinate using TPS for IMRT planning |
Lightweight plastinated phantom
Phantoms are structures made of one or more tissue substitute, and used to simulate radiation interaction in the human body (White et al., 1989). Plastination yields complex phantoms that closely represent in vivo anatomy. As early as 1988, von Hagens, the inventor of plastination, along with some of his colleagues in radiotherapy, had suggested the possibility of using plastinated phantoms for dosimetry in radiation therapy (Schmid et al., 1988). They proposed that for the plastinated phantom to simulate therapy with respect to the required dose for the patient, the physical density, atomic number, and electron density should be as similar as possible to in vivo conditions. A novel anthropomorphic plastinated pig lung phantom was developed by Yoon et al. (2008), which was stable over time and preserved the anatomical features and relative locations of the in vivo sample. The volumes for different tissue types in the phantom were comparable to the in vivo counterparts, and the CT numbers for different tissue types were within a clinically useful range. In radiotherapy, Alderson Rando phantoms are used for dosimetry in external beam treatment planning and brachytherapy treatment planning. Rando phantoms contain only skeleton, soft tissue substitute, and lung substitute, not organs (Alderson et al. 1962). Hence, anatomically accurate plastinated phantoms are desired to minimize the transitional gap between phantom studies and clinical studies caused by an overly simplified phantom like the Alderson Rando phantom (Yoon et al., 2008).
In our previous study (Shanthi et al. 2015), phantoms were made using the standard Biodur® S-10 technique, and their radiological tissue properties were compared with those of non-plastinated specimens to establish whether plastination could produce a suitable phantom for radiotherapy. It was found that the CT numbers were high, making it unsuitable for radiation dosimetry. Since the higher CT number was attributed to the denser resin, in this study, phantoms were made using the lightweight plastination technique. The xylene used in lightweight plastination mixes well with silicone and plays the role of a ‘place holder’ for air (Steinke et al., 2008), thus reducing the density of the phantom.
Radiological tissue property of the lightweight plastinated phantom
In the present study, the radiological tissue properties of the lightweight plastinates were studied. Though the CT numbers of organs in the lightweight plastinated phantom were higher than the pre-plastinates, the difference was small when compared to the standard S10 plastination technique (Shanthi et al. 2015). This is attributed to the decrease in density of the lightweight plastinated phantom. In plastination, the decrease in volume of specimens owing to shrinkage is unavoidable (von Hagens, 1985). The volume estimates in this study showed significantly less shrinkage for lungs (aerated organ), compared to our previous study, though little difference in solid organs (Shanthi et al. 2015). In this study, the radiological tissue properties such as the CT numbers and relative electron density of the lightweight plastinated phantom were comparable with the Alderson Rando phantom for soft tissue and lungs (Fig. 6).
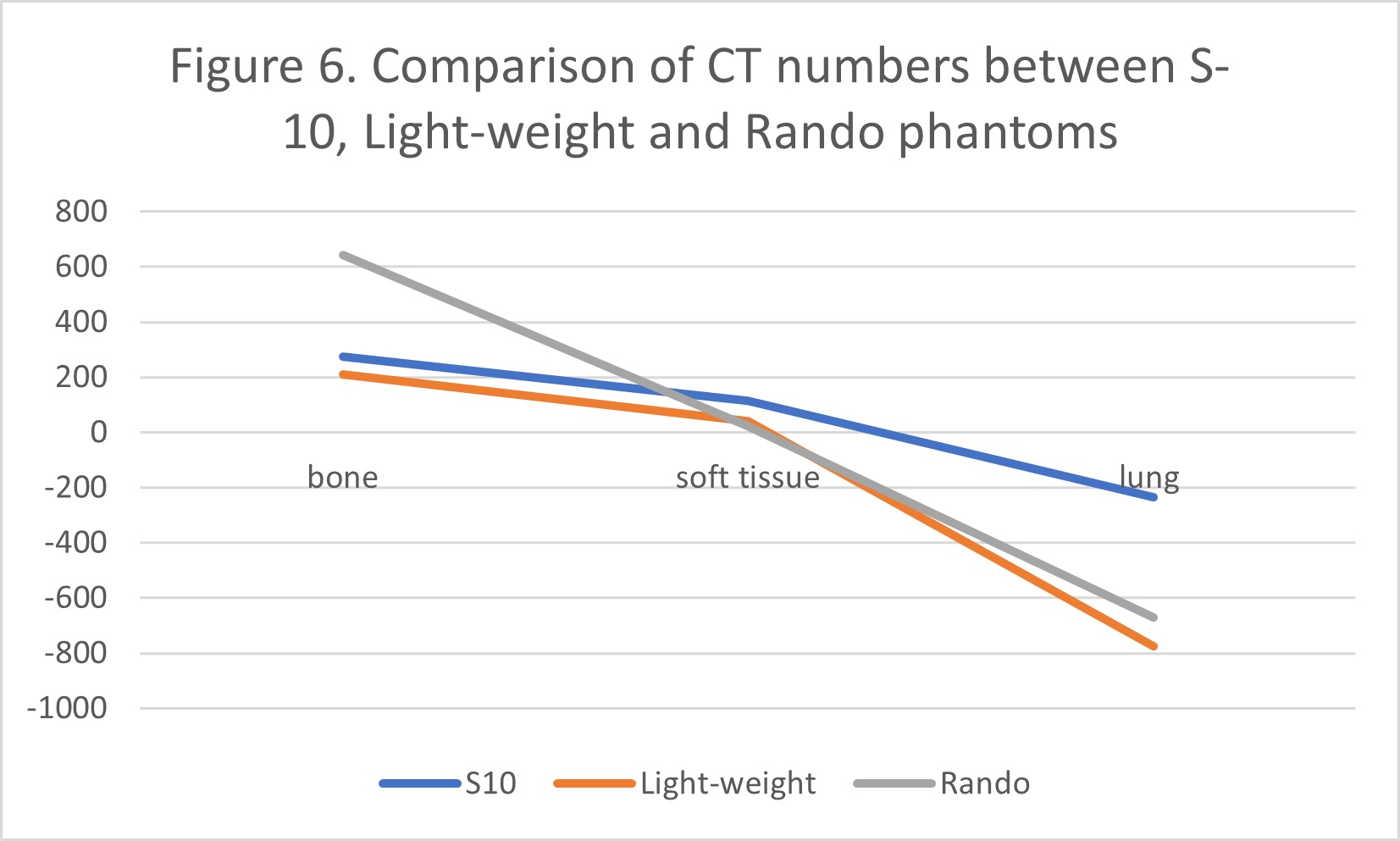 Figure 6: Comparison of CT numbers between S-10, Lightweight, and Rando phantoms. |
It was noted that the CT number for bone in the plastinated phantom was much less (211.6 in lightweight and 276.0 in S10 (Shanthi et al. 2015)), compared to the Rando phantom (644.2). Rando phantoms can have either a natural human skeleton or an artificial one made from molds. The Rando phantom used in this study had an artificial skeleton. The high CT number of bone in the Rando phantom could be attributed to the higher density of the bone substitute used.
Validation of treatment planning system (TPS) using light weight plastinated phantom
The IMRT has been established as accurate, reliable, and efficient in delivering conformal radiotherapy (Ling et al., 2008). Patient-specific quality assurance in IMRT is carried out using commercially available phantoms. This is to verify the dose calculation carried out by TPS, as this is necessary before the treatment of patients. Hence, the radiological properties of the phantom used for this purpose should be similar to that of the patient. The suitability of the lightweight plastinated phantom described here has been verified by comparing the CT numbers of various parts with that of the commercially available Rando phantom which is routinely used in quality assurance, and it was found comparable in this study. Subsequently, the light weight plastinated phantom was used for the validation of TPS. The results show that the calculated doses at PTV and various OAR were comparable to those obtained by the measurements carried out using OSL, as per the plan carried out by TPS. However, more variation was found on the right lung, although this can be considered insignificant as the variation in absolute value is minimal. Hence, the light weight plastinated phantom is more suitable when compared to the Rando Phantom as it is real human body, and, more importantly, it is cost effective.
The lightweight plastinated phantom developed in this study has radiological properties that are closer to the cadaver, which clearly explains why the variation of pre- and post-plastination specimens were within acceptable limits. The measured and calculated dose were comparable for IMRT planning. The feasibility of using epoxy plastination instead of silicon plastination for phantom development are yet to be explored.
Acknowledgements
The authors gratefully acknowledge the Fluid Research Fund, Christian Medical College, Vellore, for funding the project. We thank Dr. Leena Robinson Vimala who helped with image acquisition.
The authors sincerely thank those who donated their bodies to science so that anatomical research could be performed. Results from such research can potentially increase mankind’s overall knowledge that can then improve patient care. Therefore, these donors and their families deserve our highest gratitude.
Alderson SW, Lanzl LH, Rollins M, Spira J. 1962: An instrumented phantom system for analog computation of treatment plans. Am J Roentgenol Radium Ther Nucl Med 87: 185-195. https://www.osti.gov/biblio/4818049-instrumented-phantom-system-analog-computation-treatment-plans.
Frigo, SP. 2014: Radiation therapy dosimetry phantoms. In: DeWerd LA and Kissick M, Editors. The phantoms of medical and health physics: devices for research and development. Biological and Medical Physics, Biomedical Engineering. New York, NY: Springer, p 17-38.
https://doi.org/10.1007/978-1-4614-8304-5_2
Ling CC, Zhang P, Archambault Y, Bocanek J, Tang G, Losasso T. 2008: Commissioning and quality assurance of rapidarc radiotherapy delivery system. Int J Radiat 72 (2):575-581.
https://doi.org/10.1016/j.ijrobp.2008.05.060
Schmid H, Kimmig B, Engenhart R, Marin-Grez M, von Hagens G, Rhein B. 1988: A real anatomical specimen plastinated as a phantom for radiation therapy. British J Radiol 61(728):744-745.
Shanthi P, Singh RR, Gibikote S, and Rabi S. 2015: Comparison of CT numbers of organs before and after plastination using standard S-10 technique: radiological tissue properties of plastinates. Clin Anat 28 (4): 431-435.
https://doi.org/10.1002/ca.22514
Steinke H, Rabi S, Saito T, Sawutti A, Miyaki T, Itoh M, Spanel-Borowski K. 2008: Lightweight plastination. Ann Anat190(5):428-431.
https://doi.org/10.1016/j.aanat.2008.02.005
White DR, Booz J, Griffith RV, Spokas JJ, Wilson IJ. 1989: ICRU Report 44: Tissue substitutes in radiation dosimetry and measurements. Journal of the ICRU os23(1).
https://doi.org/10.1093/jicru/os23.1.Report44
Von Hagens G. 1985: Heidelberg plastination folder: Collection of technical leaflets for plastination. Heidelberg: Anatomiches Institut 1, Universität Heidelberg.
Yoon S, Henry RW, Bouley DM, Bennett NR, Fahrig R. 2008: "Characterization of a novel anthropomorphic plastinated lung phantom. Med Phys 35(12): 5934-43.
https://doi.org/10.1118/1.3016524