Institute of Pathology City Hospital Muenchen-Schwabing Koelner Platz 1 8000 Muenchen 40 West Germany
Two materials are used for the impregnation of brain tissue in plastination:
To produce an acceptable specimen by either technique one must begin with proper fixation. In this paper, an improved method for removing and fixing the human brain will be presented. Also included is a review of the literature dealing with brain fixation.
Fixation methods described to date have not proven suitable for preparing the human brain for plastination. Fixing a brain in a manner satisfactory for plastination requires that the specimen exhibit a natural form after fixation and that all anatomic components be completely and uniformly fixed. There should be no distortion of natural shape and no border of fixative penetration observable at the surface of a section.
Beginning with methods described in the literature, the author has developed a procedure to fulfill these demands. This procedure has been used for four years and has yielded consistently acceptable results.
Brain; P35; Epoxy; Silicone; Biodur; S10
Alfred Riepertinger Institute of Pathology City Hospital Muenchen-Schwabing Koelner Platz 1 8000 Muenchen 40 West Germany

![]()



Two materials are used for the impregnation of brain tissue in plastination:
To produce an acceptable specimen by either technique one must begin with proper fixation. In this paper, an improved method for removing and fixing the human brain will be presented. Also included is a review of the literature dealing with brain fixation.
Fixation methods described to date have not proven suitable for preparing the human brain for plastination. Fixing a brain in a manner satisfactory for plastination requires that the specimen exhibit a natural form after fixation and that all anatomic components be completely and uniformly fixed. There should be no distortion of natural shape and no border of fixative penetration observable at the surface of a section.
Beginning with methods described in the literature, the author has developed a procedure to fulfill these demands. This procedure has been used for four years and has yielded consistently acceptable results.
Although it was developed for plastination, it is completely applicable to the routine fixation of autopsy specimens. The procedure begins with fresh tissue. No fixation is performed in situ. The untreated brain is removed and the body turned over to the undertaker.
A human brain in the fresh state is unable to retain its shape without support, hence, once removed from the cranium, it must be transferred to a special, cranium-shaped vessel which will sustain it properly and determine its form during the steps to follow. We refer to this container as a "hedgehog mold." Use of a hedgehog mold permits immediate release of the body and allows subsequent steps to be performed slowly, thereby reducing the potential for specimen damage.
REMOVAL OF THE BRAIN
In removing the brain, the calvarium is exposed and the cap of the skull is cut away with the usual, circumferential incision. This incision is made with a circular saw, having a blade diameter of 5 cm. The blade is equipped with a plate that limits the depth of the cut to 0.4 cm. Since the thickness of the skull varies from one area to another, caution must be exercised. The depth-limiting plate cannot be relied on completely to protect
underlying structures. The depth of the cut must be regulated, by hand, to prevent damage to the brain.
Final removal of the cranial cap is accomplished with a cross-pledget. Again, great care must be exercised. This instrument is gripped lightly and used with minimum pressure to avoid penetration of the brain. At intervals of approximately 2 cm the bony cap is chiseled from its attachment and removed. The exposed dural surface may now be inspected for damage. With surgical forceps, the dura mater is then carefully lifted from the cerebral hemispheres and, using a pointed scissors, it is cut along the line of incision. The falx cerebri at the front of the brain is severed with slightly opened scissors and the dura is reflected, as far as possible, toward the middle of the brain. This is necessary to avoid rupturing a vessel.
The next step is to remove the brain. During this entire process, the occipital lobes must be supported with one hand while the other is used to free the brain from the cranial fossae. First, the olfactory nerves are gently detached by elevating them from the frontal base of the skull, using light pressure on the underside of the anterior brain. Next, the optic nerves, which are now under tension, can be cut. This is followed by cutting both carotid arteries, the tuberal hypophysis and the oculomotor nerves.
Next, both temporal lobes are freed from their cavities using blunt dissection with the fingers. The tentorium cerebelli should now be visible and both sides may be cut along the petrous portions of the temporal bone, using a long, pointed knife. The cut should be performed in a mediolateral direction. Once the tentorium has been cut, the cerebellum can be gently pushed back, away from the temporal lobes.
A long, thin knife is now used to cut around the spinal cord as it passes through the foramen magnum. The spinal cord is then transected as far as possible into the spinal canal. Supporting the cerebellum, the brain and remaining spinal cord are now gently lifted out of the cranium and placed in the hedgehog mold.
FIXATION OF THE HUMAN BRAIN: A BRIEF REVIEW OF THE LITERATURE
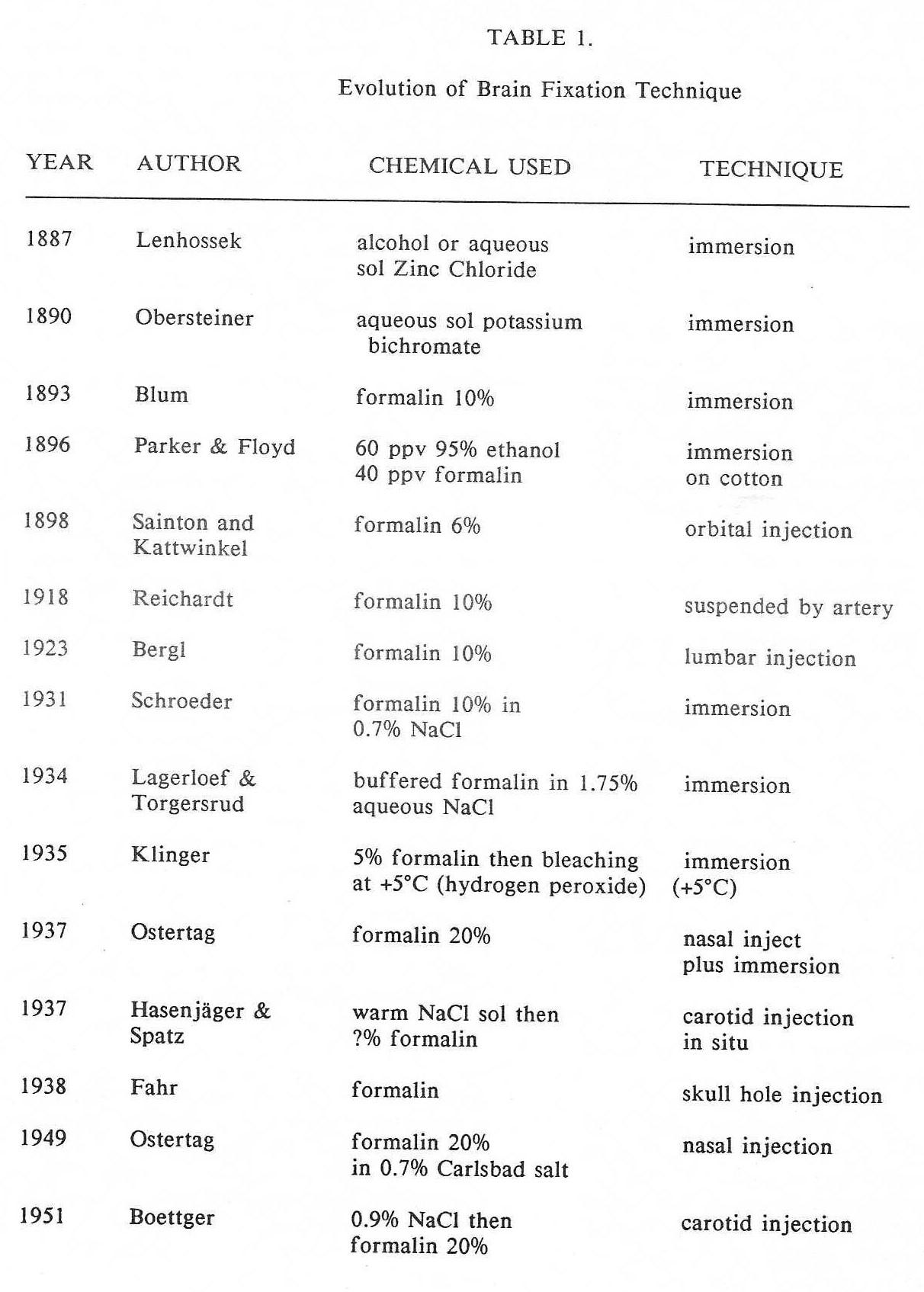
Table 1 - Evolution of Brain Fixation Technique
Table 1. provides a summary of the most important historical steps in the evolution of brain fixation techniques. Before the advent of formaldehyde in 1893, ethanol or an aqueous solution of zinc chloride or potassium chloride was used. Blum introduced formalin as a preservative of biological specimens. In his very first publication (1893) he recommended fixation of brain tissue by immersion in 10% formalin.
Two categories of opinion seem to prevail in current literature. Some authors recommend immersion alone as an adequate means of fixation; others favor injection in situ, followed by immersion. With regard to injection, some prefer to introduce fixative into the subarachnoid space; others favor using the carotid arteries. Subarachnoid injection has been performed via a lumbar, nasal or orbital approach or by drilling a hole into the cranial cavity. Carotid injection may be done within the skull, at the site where the internal carotid arteries enter the brain (Hasenjaeger and Spatz) or at the neck as they branch from the common carotid arteries (Boettger). All three authors emphasize the necessity of saline injection before formalin injection and of immersion of the brain in a formalin solution following injection.
Since 1931, it has been suggested by many authors that an isotonic solution of potassium chloride should be used in the preparation of formalin fixative. Schroeder claims that, if 0.9% potassium chloride is used, brain tissue will remain dimensionally stable during fixation. Without potassium chloride, he found that swelling of about 15% is inevitable. Several other authors have recommend the use of isotonic sodium chloride for this same reason, in both immersion and injection.
Since its recommendation by Klinger in 1935, most laboratories immerse the human brain in 5% formalin for fixation. As advised in 1918 by Reichardt, many laboratories also suspend the brain by a basilar artery during immersion.
Brain fixation techniques in common practice today have three basic disadvantages:
1. None incorporate a means for support of the fresh brain. Fixation must be done outside the body, starting with fresh tissue. Although in-situ fixation is highly desirable, it is usually not possible in the routine autopsy because of time limitation.
2. The natural shape of the brain is often deformed during extracranial fixation.
3. No currently practiced method permits complete fixation of a fresh brain, once it has been removed from the skull.
In the remaining sections of this paper, specific recommendations for overcoming these problems will be presented.
RECOMMENDATIONS FOR BRAIN FIXATION
The first step after removal of a fresh brain is to transfer it to a hedgehog mold for establishment of a near-natural form. (Incidentally, a hedgehog is a small, brain- shaped animal, found in great numbers in Europe. The hedgehog mold is so named because its general outline bears a reasonable resemblance to this animal.) The hedgehog mold has a capacity of 1300 ml and weighs 290 grams. It is possible, therefore, to weigh the brain while it is contained in this vessel. At our institute, a brain remains within this mold during the clinical conference which is held 2 or 3 hours after autopsy. Immediately after the conference, fixation is begun.
A catheter is inserted into one vertebral artery until its tip has entered the basal artery. The second vertebral artery and both internal carotid arteries are clamped off and 150 ml of 100% formalin is gently injected. After a few hours, the brain is immersed, suspended by a basilar artery, in about 4 liters of 5% formalin, where it remains for one week.
USE OF 100% FORMALIN AS A PRE- IMMERSION INJECTION
The use of 100% formalin for pre- immersion injection was determined by an experiment, performed by the author. In summary, the following comparisons were made:
1. 12 brains were fixed by simple suspension in 5% formalin and 12 brains were injected with 100% formalin and then immersed in 5% formalin. Four brains from each group were cut after three hours and four after one week.
2. Sections were compared for adequacy of fixation and both groups were further compared to others that had previously been prepared by injection of various dilutions of formalin, followed by immersion.
Injection with 100% formalin prior to immersion resulted in a far superior specimen than either simple immersion or injection with diluted formalin followed by immersion. The use of isotonic saline or plasma expander solutions as a pre-injection rinse did not offer any advantage nor did it improve the results.
Injection of 100% formalin led to complete fixation in one week, about half the time needed when the brain was fixed by immersion alone. The contrast between white and gray matter was improved and large histologic sections adhered much better to a slide.
PREPARATION OF THE FIXED BRAIN FOR DEHYDRATION
After an immersion time of one week, the dura is removed and the brain rinsed with tap water for about 30 minutes. At this stage, it is advisable to check for symmetry and for damage incurred while opening the skull. Acceptable specimens are then immersed in a freshly-prepared, 5% solution of formalin and kept at refrigerator temperature (+5°C) for 24 hours. This step is required to prevent ice crystal formation during freeze- substitution (dehydration). Basilar artery suspension is not necessary during this immersion.
SUMMARY OF THE PROCEDURE RECOMMENDED FOR FIXATION OF THE BRAIN
1. Open the skull, remove the brain and transfer it immediately to the hedgehog mold.
2. Prepare injection instruments and 100% formalin for injection.
3. Insert a cannula into the vertebral artery and clamp off the remaining vertebral artery and both internal carotid arteries.
4. Inject about 150 ml of 100% formalin into the brain.
5. Prepare about 5 to 5.0 liters of 5% formalin in a suitable container.
6. Suspend the injected brain, immersed in the 5% formalin, by a basilar artery for one
none