1 Department of Integrative Biology and Physiology, University of Minnesota, Medical School, Minneapolis, MN 55455, USA.
2 Anatomy Bequest Program, University of Minnesota, Medical School, Minneapolis, MN 55455, USA.
The purpose of this study was to develop a plastinated model of a male and female pelvis that could be manipulated to allow students to remove organs, blood vessels and nerves from the pelvis. The pelvis of one male (70 years old) and one female (75 years old, para 2), with no known pelvic surgery or disease, were dissected by removing the organs, major arterial trunks and sacral nerves individually. All of the soft tissue was removed from the bony pelvis in each, except for the muscles of the pelvic floor, obturator membrane, sacrotuberous ligaments and sacrospinous ligaments. The erectile tissues were also dissected and removed en bloc. The pelvic components were then plastinated to replace the tissue fluids with silicone. The resulting plastinated pelvic models accurately represent the anatomy of the male and female pelvis, with removable parts. The dissection and plastination technique require a skilled dissector, a plastination lab, and can be repeated as necessary to represent desired pelvic anatomy variability. The plastinated pelvic models also resulted in excellent scanned images that were then used to print 3D models.
anatomy; education; model; pelvis; plastination
Dr. Mark S. Cook, Department of Integrative Biology and Physiology, University of Minnesota, Medical School, Minneapolis, MN 55455, USA. Tel.: +001 612 626 5040; Fax.: +001 612 301 1543; E-mail: cookx072@umn.edu.

![]()



Understanding the three-dimensional (3D) anatomy of the human body is a critical component of first-year medical education. Many clinical tasks and procedures require a firm understanding of spatial relationships between closely associated structures (Cottam, 1999; Garg et al., 2001). This is especially true for one of the more complex areas of the body, the pelvis. Pelvic issues, in general, make up a significant percentage of patients scheduling visits with their physicians. This is true in both males and females. It is estimated that 25% of women in the United States are affected by urinary incontinence, fecal incontinence and pelvic organ prolapse (Nygaard et al., 2008). In men, prostate cancer is the second most common cause of death (Halpern et al., 2003). It is important for medical students to acquire a very good understanding of pelvic anatomy to effectively treat pelvic conditions in their future patients with minimal disruption to nearby unaffected structures. Understanding the 3D anatomy of the pelvis is also essential for interpreting medical imaging.
Cadaveric dissection is a key teaching component in the anatomy laboratory at the University of Minnesota. This is where students have the opportunity to not only learn anatomy, but understand it through discovery. Dissection has withstood the test of time as an effective teaching tool because it allows students to discover the 3D relationships of the structures of the body through the use of multiple senses (Sugand et al., 2010; DeHoff et al., 2011). Dissection also exposes the wide variety of anatomical variation seen in the general (donor) population. However, when it comes to the pelvis, students are often frustrated with the dissection process because of the layering of structures and organizational complexity in this region. It is notoriously one of the most challenging dissections students face. In order to alleviate some of the pressures during the pelvic dissection laboratory, prosections performed by the anatomy faculty have become important teaching aids that students depend on for understanding this region of the body. However, the time-consuming dissections required to meet the demands of a 175-student class are short-lived, being removed from the laboratory and cremated at the end of each semester. Silicone plastination, in which tissue fluid is replaced with a curable polymer (von Hagens, 1979a; 1979b; 1986), was considered as an option for preserving the carefully dissected pelvic specimens. However, the resulting plastinated model would significantly reduce the ability of students to mobilize structures to inspect surrounding anatomy. This dilemma led to the development of the dissection and plastination method described in this current report. The method described here allows for the creation of plastinated pelvic dissections that allow students to remove organs, blood vessels and nerves individually. Taking advantage of the flexibility of the model described here, it is also possible for students to approach pelvic anatomy through “syncretion,” a term coined by Miller (2000) for anatomical discovery by “putting things back together again.” To our knowledge, this is the first description of the development of a male and female plastinated pelvis model that allows students to “build a pelvis” by inserting organs, blood vessels and nerves into the pelvic cavity with the pelvic floor muscles intact.
Pelvic dissections were performed on one male and one female human cadaver. The cadavers were gratefully donated to the Anatomy Bequest Program, at the University of Minnesota. The cadavers were first embalmed with a solution of 70% isopropyl alcohol, 13.25% phenol, 8% sorbitol, 7.5% formaldehyde and 1.25% barquat MB-50 diluted in water (50:50). The female cadaver was 75 years old with a history of two live births. No pelvic surgeries or anomalies were noted. The body was prepared for dissection by isolating the pelvis. A horizontal cut was made through the body at the L3 vertebral level. The lower extremities were then sectioned horizontally through the upper thighs. The pelvic viscera were then dissected with the urinary bladder, uterus, rectum, pelvic nerves and major arterial trunks removed separately. The erectile tissues of the external genitalia were then dissected and removed en bloc. Finally, the bony pelvis was cleaned of all soft tissue except for the pelvic floor muscles and major ligaments. The pelvic components were then plastinated.
The male cadaver was 70 years old, with no significant medical history involving the pelvis. As with the female cadaver, the male body was prepared for dissection by sectioning horizontally at the L3 vertebral level and at the upper thighs. The pelvic viscera were then dissected, with the urinary bladder, rectum, pelvic nerves and major arterial trunks removed separately. The testes and vasa deferentia were removed with the bladder. The erectile tissues of the penis were then dissected and removed en bloc. Finally, the bony pelvis was cleaned of all soft tissues except for the pelvic floor muscles and major ligaments. The pelvic components were then plastinated.
The plastination process employed is referred to as “room temperature plastination.” In contrast to the basic cold process, which combines a silicone polymer with a catalyst and chain extender to serve as the impregnation mixture (von Hagens, 1986), the room temperature method combines the silicone polymer with a cross-linker (Glover et al., 1998). This method produces a more stable impregnation-mix at room temperature compared to the cold method. The specific materials and methods used to prepare the plastinated pelvis models in our study are comparable to techniques previously described (Henry, 2007; Raoof, 2007). However, North Carolina products were used based solely on familiarity and availability.
Plastination Process
The resulting pelvic plastinate models included parts that could be placed within, or removed from, the pelvic cavity.
Eight Parts of Female Pelvic Model:
 (A) anterior view 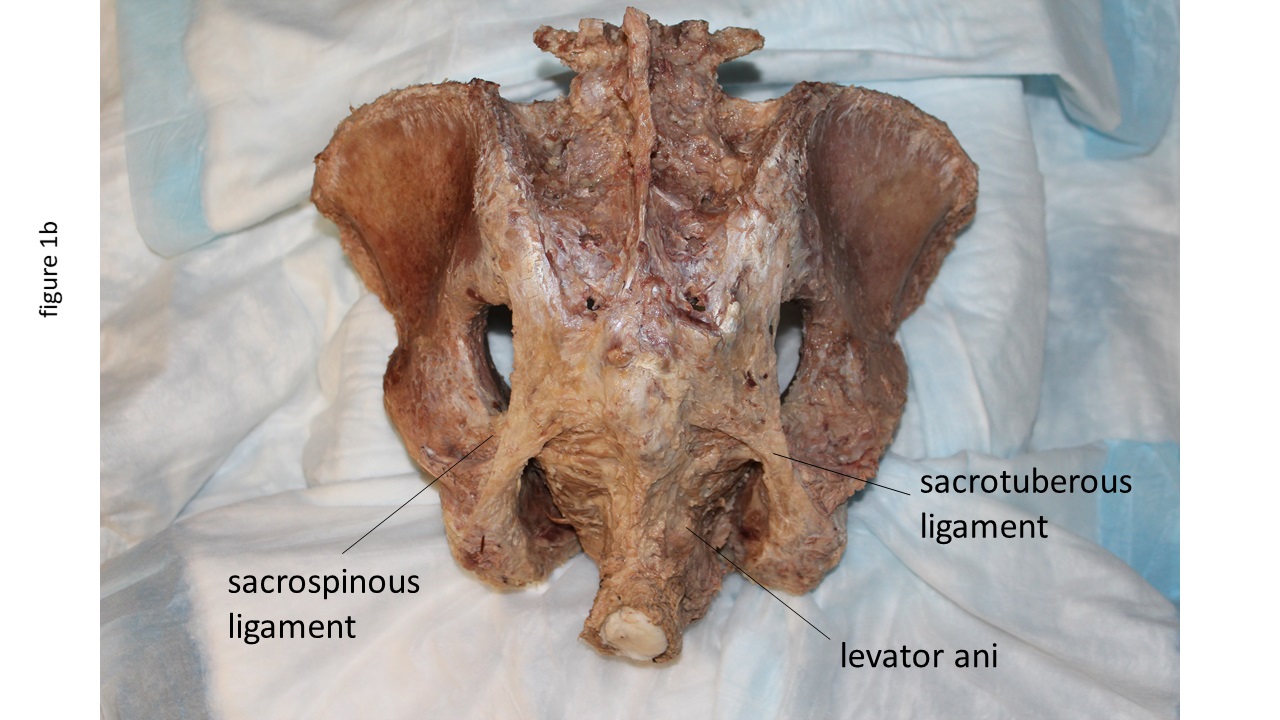 (B) posterior view  Figure 1. Plastinated female pelvis with ligaments and pelvic floor muscles from an anterior view (A), posterior view (B) and superior view (C). |
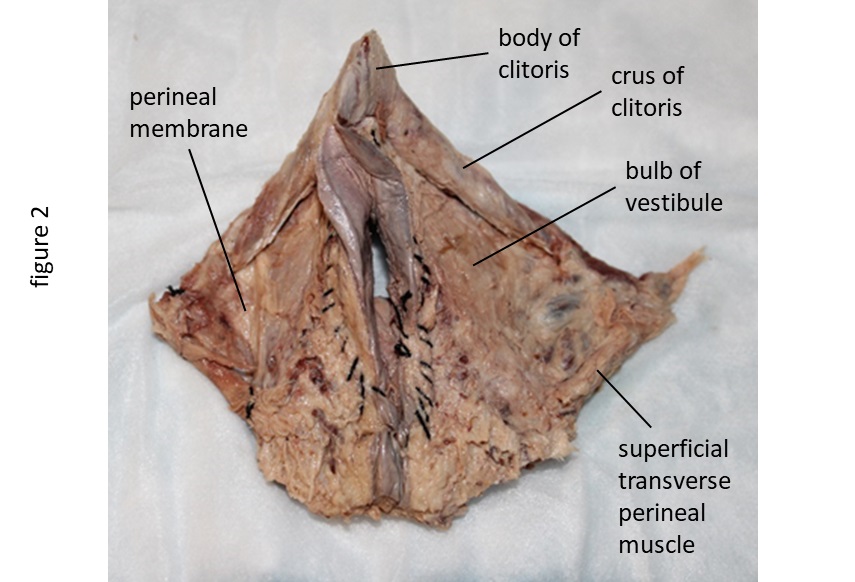 Figure 2. Anterior view of plastinated female external genitalia. |
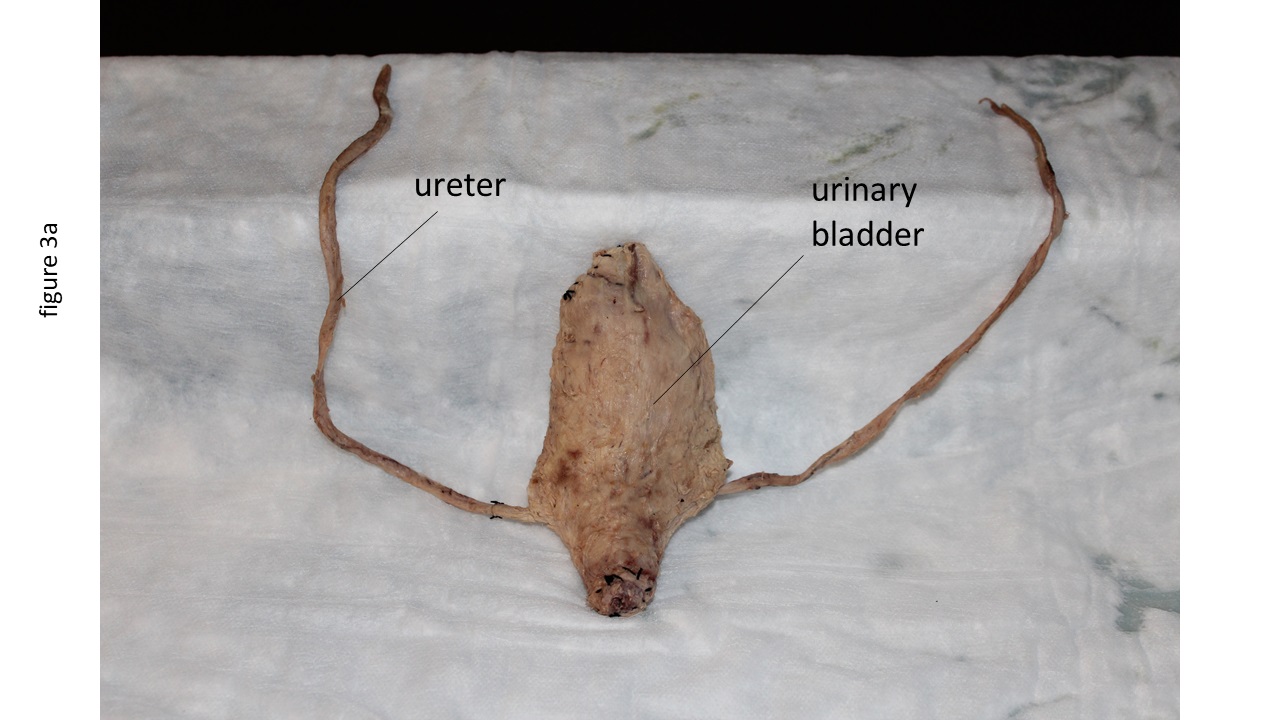 (A) anterior view of bladder  (B) anterior view of uterus  Figure 3. Plastinated female pelvic organs, including anterior view of bladder (A), anterior view of uterus (B) and lateral view of rectum (C). |
 Figure 4. Anterior view of plastinated arterial branches (A) and sacral nerves (B). |
 Figure 5. Anterior view of assembled female pelvis plastinate. |
Seven Parts of Male Pelvic Model:
In order to maintain the natural shape and position of the various pelvic components during plastination, the various pelvic structures were pinned into position or suspended by wires at the start of plastination (Fig. 11) but were removed from the pelvic cavity after impregnation.
 (A) anterior view 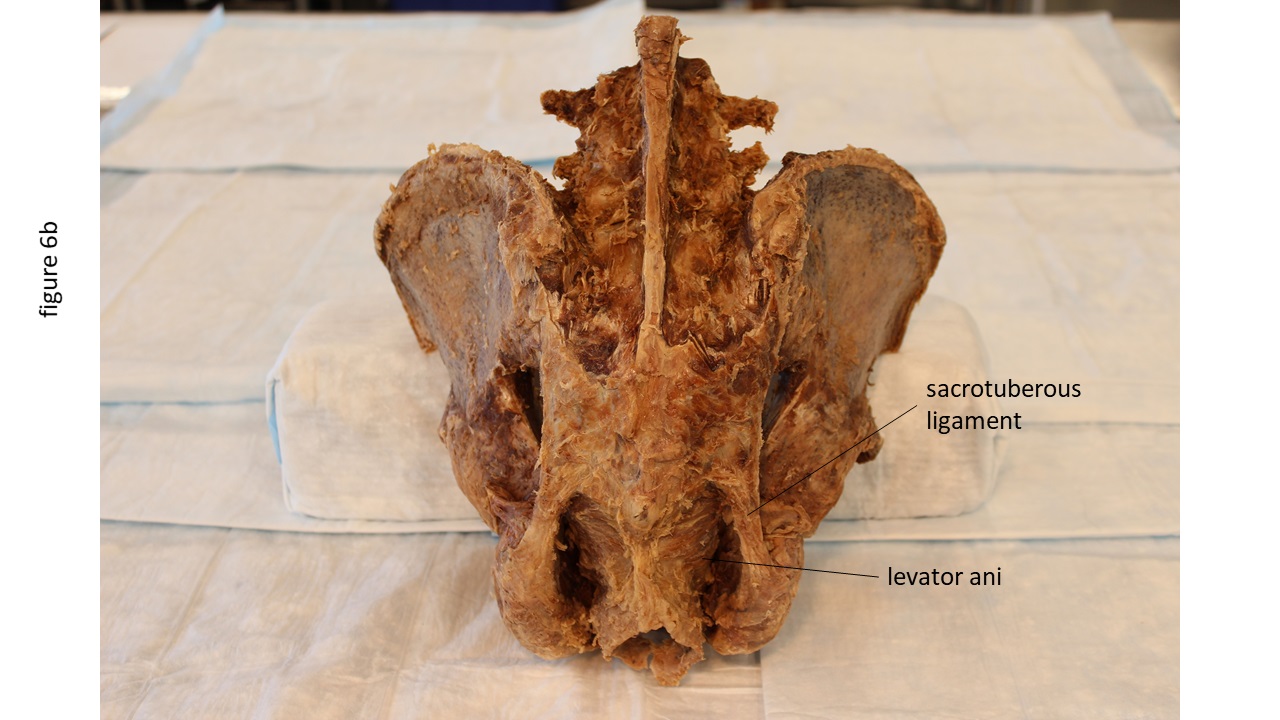 (B) posterior view 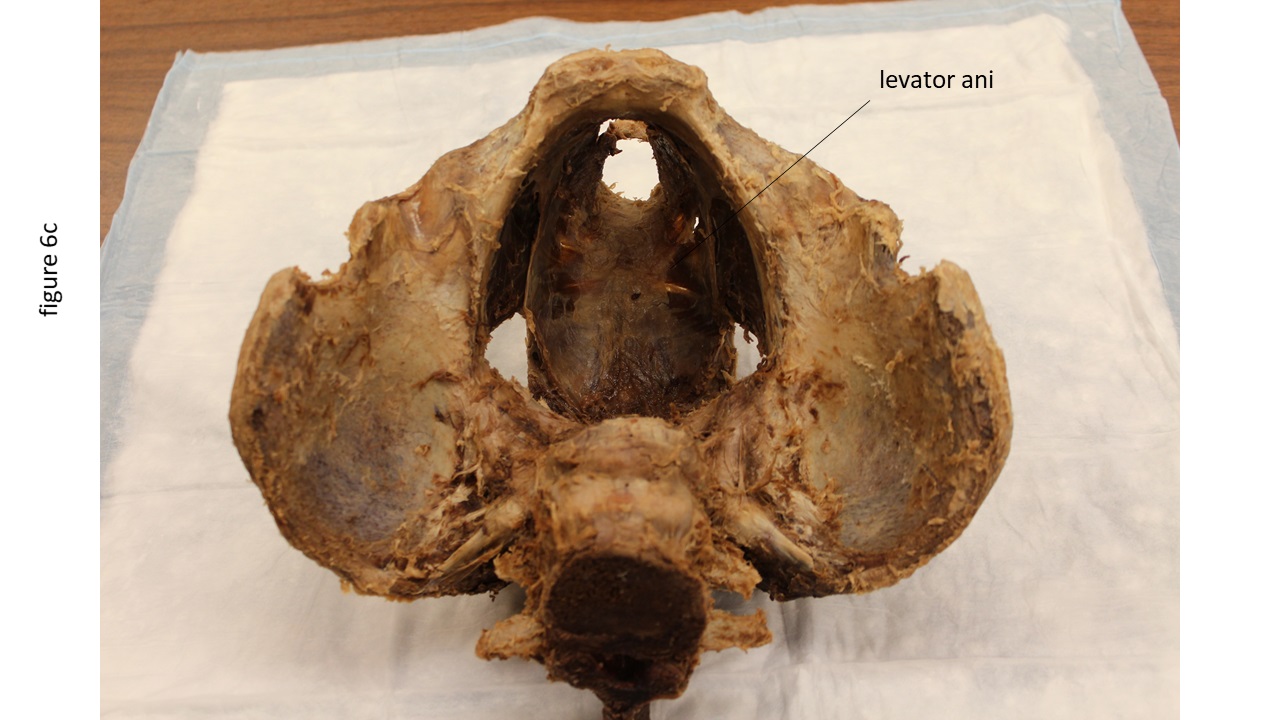 Figure 6. Plastinated male pelvis with ligaments and pelvic floor muscles from an anterior view (A), posterior view (B) and superior view (C). |
 Figure 7. Left lateral view of plastinated male erectile tissues. |
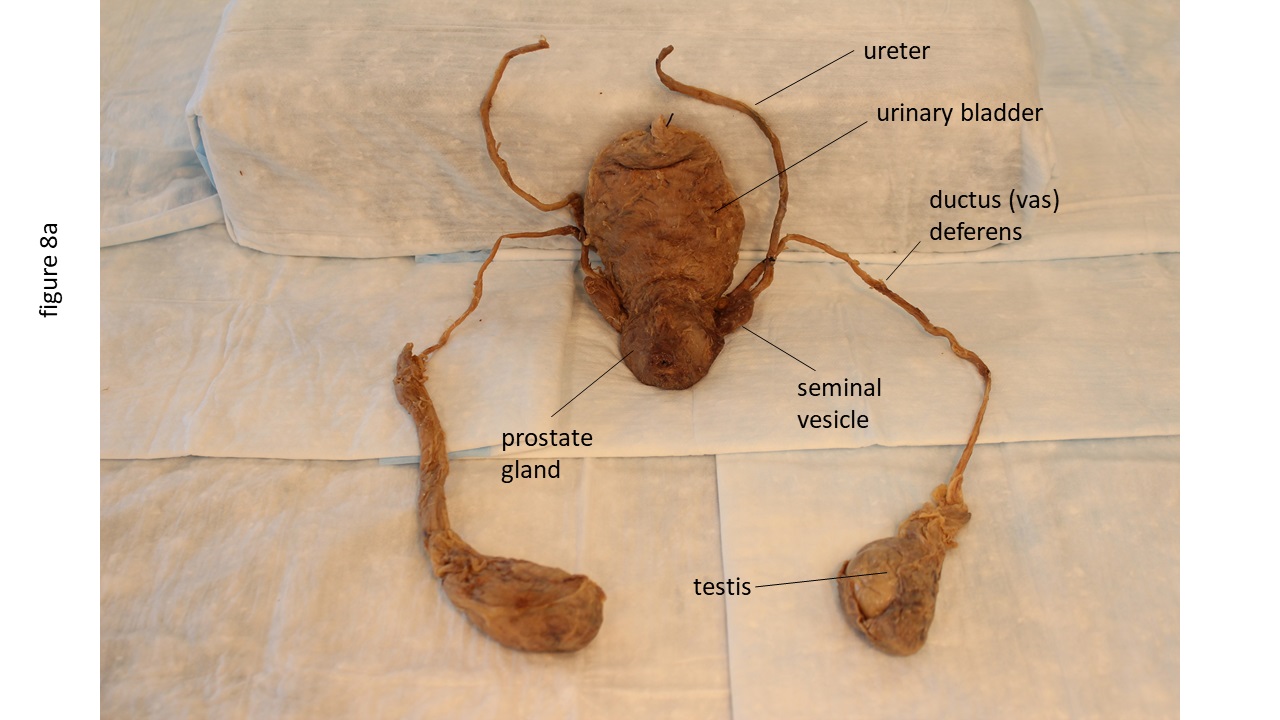 (A) anterior view of plastinated bladder with male reproductive structures  Figure 8. Anterior view of plastinated bladder with male reproductive structures (A) and lateral view of rectum (B). |
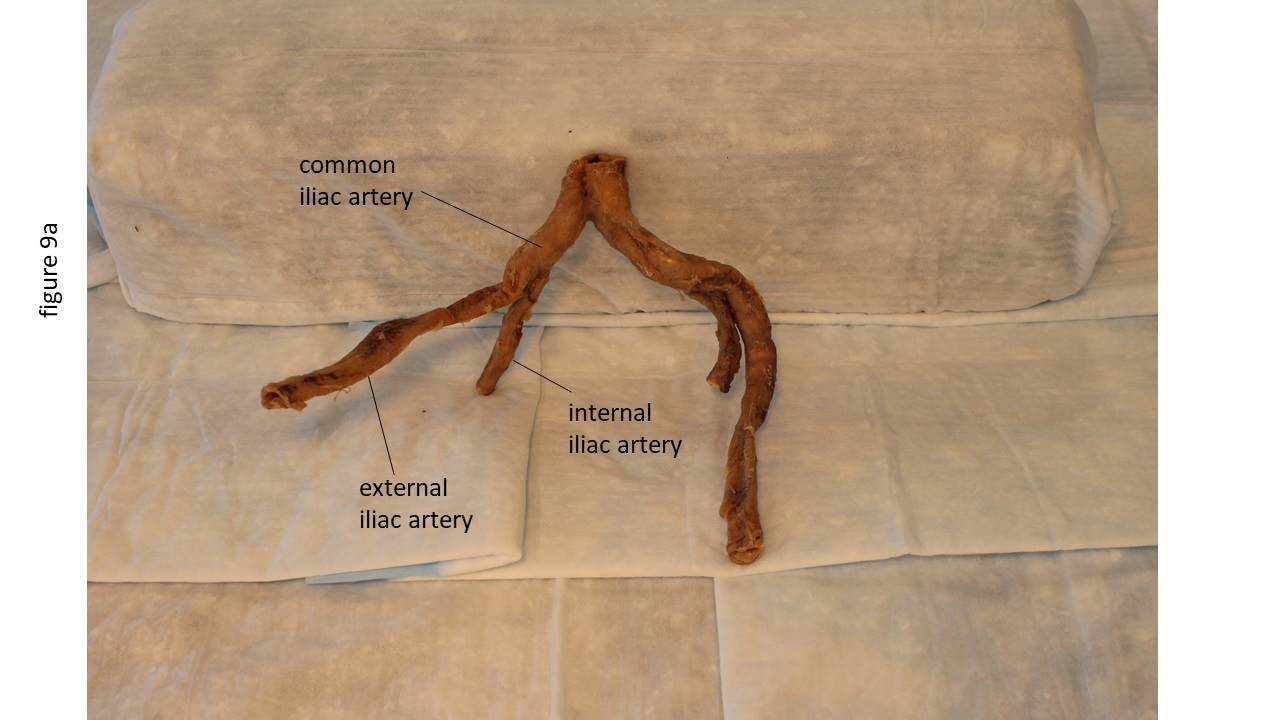 (A) anterior view of plastinated arterial branches
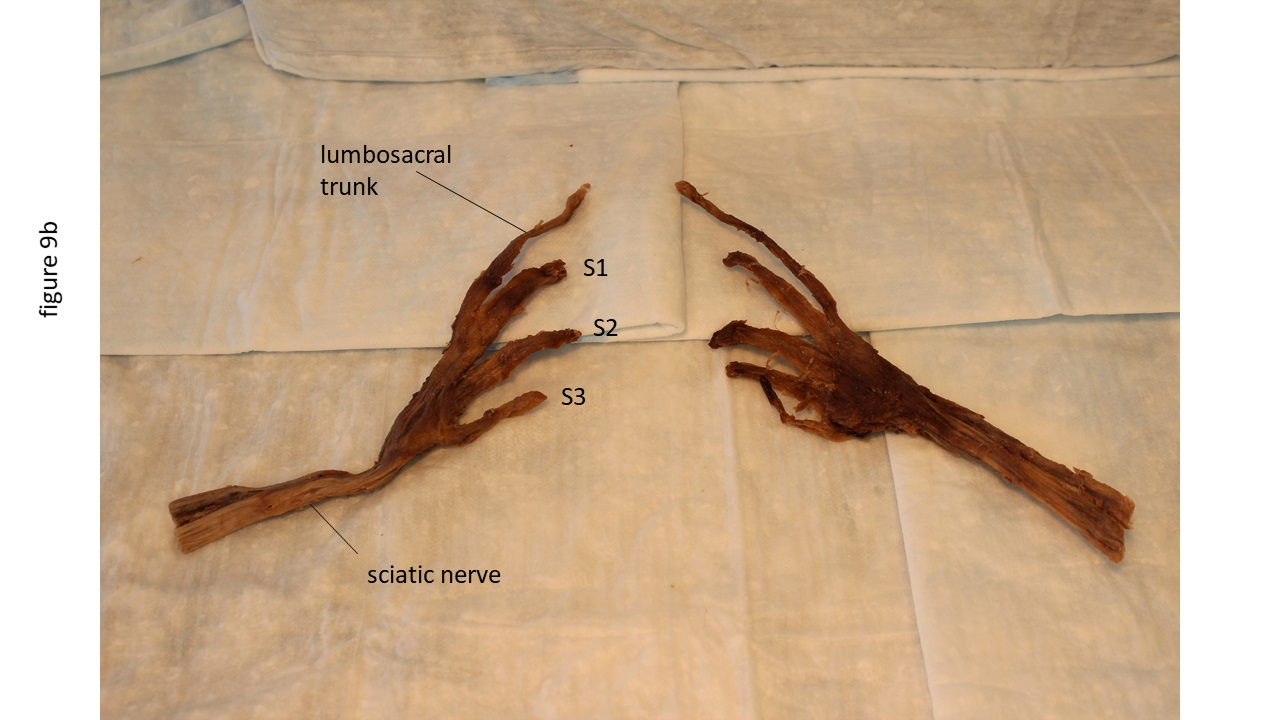 Figure 9. Anterior view of plastinated arterial branches (A) and sacral nerves (B). |
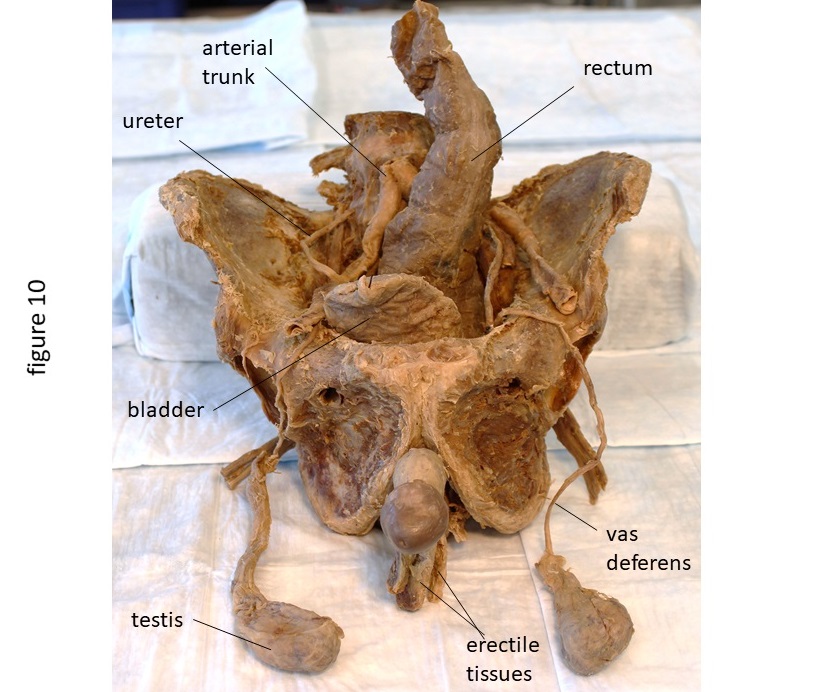 Figure 10. Anterior view of assembled male pelvis plastinate. |
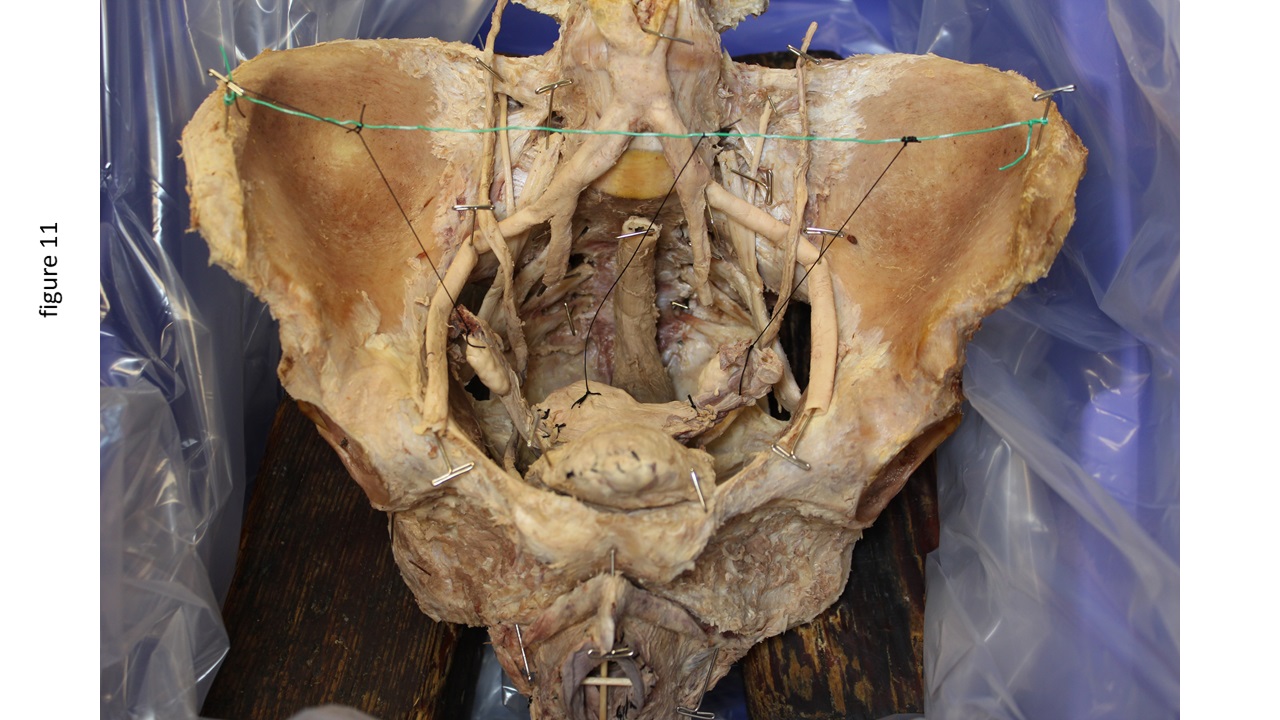 Figure 11. Female pelvic components pinned and suspended in pelvic cavity in preparation for plastination. |
Although a formal experience survey was not administered, students have commented that the pelvic plastinate models “really helped” with the understanding of pelvic anatomy, was “a fun way to learn pelvic anatomy,” and provided for “immediate comprehension” of the organization of pelvic contents.
To our knowledge, this is the first description of a process by which the male and female pelvis can be dissected and plastinated to allow organs, blood vessels and nerves to be removed individually, or placed into the pelvis to “build a pelvis.” Other types of models can be used to help teach pelvic anatomy. Plastic models have been used in anatomy courses for decades to help students understand the structure of the body. They may be sufficient for an introductory anatomy course, but tend to lack the detail, accuracy and interactive qualities that are desirable for more advanced courses such as medical anatomy. This is especially true for the pelvis. For example, the robustness of the levator ani muscle (the main muscle of the pelvic floor) is overly represented in most plastic models. In reality, the muscle is usually very thin and disrupted with regions of the connective tissue. In addition, plastic models lack the interactive nature desired by students. Many times, several organs are represented in a single mass, limiting a student’s spatial understanding. It is clear that a student’s spatial ability is an important predictor of success in learning anatomy (Garg et al., 2001).
There has also been a rise in the popularity of computer-generated 3D models of the pelvis. Computer models and animations of anatomical features are becoming increasingly attractive as a means to communicate complex spatial relationships effectively (Dev et al., 2002). Virtual models of the pelvis are typically produced from cross-sectional images (Bajka et al., 2004; Holubar et al., 2009; Sergovich et al., 2010; Wu et al., 2010; Sora et al., 2012; Kraima et al., 2013; Sora and Jilavu, 2013). Earlier studies questioned the efficacy of such models with helping students perform better on exams (Garg et al., 2002; Hariri et al., 2004) and suggested that they may actually handicap those students with poor spatial ability (Garg et al., 1999). However, more recent studies have shown that they are beneficial to anatomy students (Qayumi et al., 2004; Nicholson et al., 2006; Brown et al., 2012; Cui et al., 2017), which may be due to the much-improved quality of computer-generated modeling.
These virtual models, however, require a great amount of time and expertise to create. They must have the boundaries of each structure rendered slice by slice by an expert in anatomy and with proficiency using the software. The process, called “segmentation,” is the digital identification and labeling of structures of interest on individual two-dimensional (2D) slices. This process must be completed in several planes for tortuous structures such as blood vessels. A major problem for segmentation arises from the separation of ligaments and connective tissue from bones and muscles, because structures merge directly into one another (Bajka et al., 2004). The definition of the borders of individual structures is left to the discretion of the software user. The resulting model is an interpretation of 2D sectional anatomy. Secondly, the final 3D model lacks realistic tissue texture. This is because the rough form of the digital model usually undergoes further processing, such as “smoothing” to become more presentable and portable (Sergovich et al., 2010). The smoothing process results in the loss of detail and surface texture.
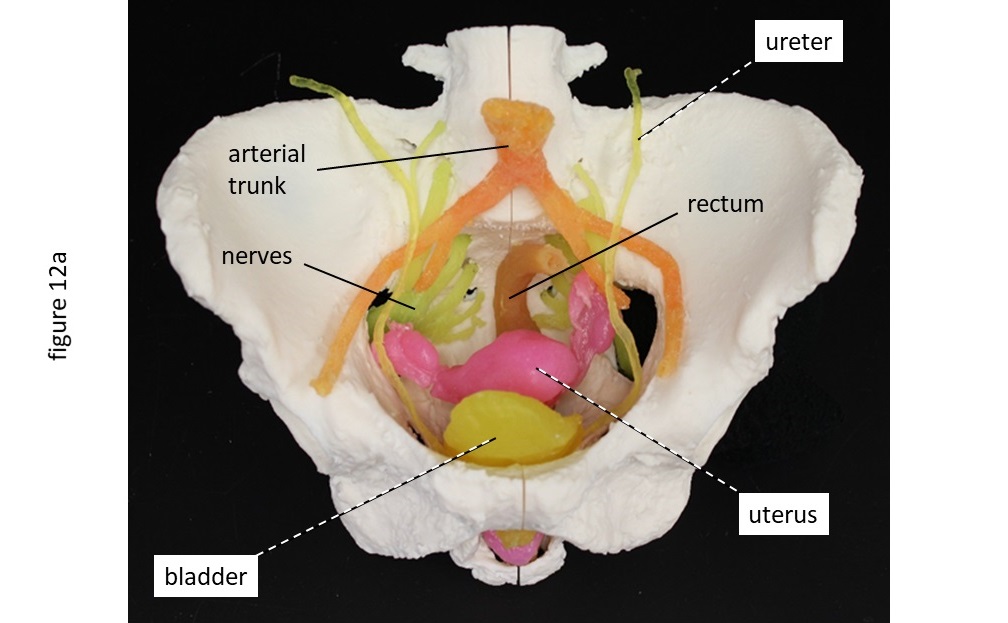 (A) assembled 3D print of whole female pelvis 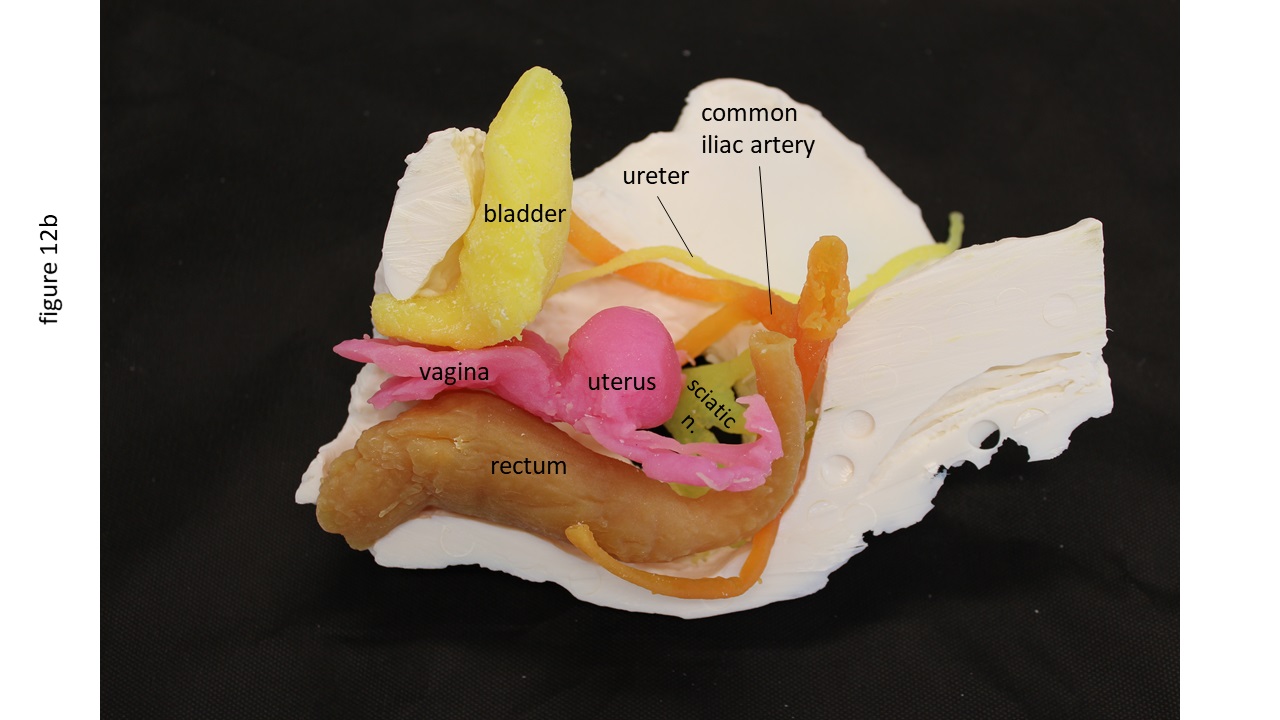 Figure 12. Assembled 3D print of whole female pelvis (A) and hemisection view (B). |
The process described in our current report does not require expensive, high-tech equipment or software. The plastination process cost approximately $1400 to perform for both pelves. It does, however, require the skill of dissection and plastination capabilities. There is no “guess-work” or “interpretation” involved, but simply revealing the structures in their true form. All of the detail and surface textures of the structures are retained. The technique can be used to preserve unlimited variations of pelvic anatomy with the level of detailed limited only by the person performing the dissections. They can be left natural in color or painted to make structure identification easier. The plastinated models described in this report also work very well for creating 3D printed models, of which the plastination process is a critical step. Once plastinated, the pelvic models’ components hold their shape when being scanned and can be placed directly on the scanning table without special containment or ventilation. Once scanned, the image files are converted to a compatible format for 3D printing. The various components of the models can also be printed in different colors and planes for ease of identification (Fig. 12). If developing colored 3D prints is not feasible, the plastinates can be painted for easier identification.
While the development of innovative learning resources should be actively encouraged, their incorporation into medical education should include quantitative evidence supporting their efficacy at improving students’ knowledge and understanding. We plan on moving forward by determining the utility of our plastinated pelvic models by evaluating student performance in a measurable way.
Bajka M, Manestar M, Hug J, Szekely G, Haller U, Groscurth P. 2004: Detailed anatomy of the abdomen and pelvis of the visible human female. Clin Anat 17:252-260.
https://doi.org/10.1002/ca.10215
Brown PM, Hamilton NM, Denison AR. 2012: A novel 3D stereoscopic anatomy tutorial. Clin Teach 9:50-53.
https://doi.org/10.1111/j.1743-498X.2011.00488.x
Cottam WW. 1999: Adequacy of medical school gross anatomy education as perceived by certain postgraduate residency programs and anatomy course directors. Clin Anat 12:55-56.
https://doi.org/10.1002/(SICI)1098-2353(1999)12:1<55::AID-CA8>3.0.CO;2-O
Cui D, Wilson TD, Rockhold RW, Lehman MN, Lynch JC. 2017: Evaluation of the effectiveness of 3D vascular stereoscopic models in anatomy instructor for first year medical students. Anat Sci Educ 10:34-45.
https://doi.org/10.1002/ase.1626
DeHoff ME, Clark KL, Meganathan K. 2011: Learning outcomes and student-perceived value of clay modeling and cat dissection in undergraduate human anatomy and physiology. Adv Physiol Educ 35:68-75.
https://doi.org/10.1152/advan.00094.2010
DeJong K, Henry RW. 2007: Silicone plastination of biological tissue: Cold-temperature Technique BiodurTM S10/S15 technique and products. J Int Soc Plastination 22:2-14.
https://doi.org/10.56507/ZLMJ7068
Dev P, Montgomery K, Senger S, Heinrichs WL, Srivastava S, Waldron K. 2002: Simulated medical learning environments on the internet. J Amer Med Informatics Assoc 9:437-447.
https://doi.org/10.1197/jamia.M1089
Garg AX, Norman G, Spero L, Taylor I. 1999: Learning anatomy: Do new computer models improve spatial understanding? Med Teach 21:519-522.
https://doi.org/10.1080/01421599979239
Garg AX, Norman GR, Sperotable L. 2001: How medical students learn spatial anatomy. Lancer 357:363-364.
https://doi.org/10.1016/S0140-6736(00)03649-7
Garg AX, Norman GR, Eva KW, Spero L, Sharan S. 2002: Is there any real virtue of virtual reality? The minor role of multiple orientations in learning anatomy from computers. Acad Med 77:S97-LS99.
https://doi.org/10.1097/00001888-200210001-00030
Glover R. 2004: Silicone plastination, room temperature methodology: Basic techniques, applications and benefits for the interested user. Abstract presented at The 12th International Conference on Plastination, Murcia, Spain July 11-16, 2004. J Int Soc Plastination 19:7.
Halpern EJ, McCue PA, Aksnes AK, Hagen EK, Frauscher F, Gomella LG. 2003: Contrast-enhanced US of the prostate with Sonazoid: Comparison with whole-mount prostatectomy specimens in 12 patients. Radiol 226(1)361-366.
https://doi.org/10.1148/radiol.2222010582
Hariri S, Rawn C, Srivastava S, Youngblood P, Ladd A. 2004: Evaluation of a surgical simulator for learning clinical anatomy. Med Educ 38:896-902.
https://doi.org/10.1111/j.1365-2929.2004.01897.x
Henry RW. 2007: Silicone plastination of biological tissue: Room-temperature technique North Carolina technique and products. J Int Soc Plastination 22:26-30.
https://doi.org/10.56507/FSNZ3092
Holubar SD, Hassinger JP, Dozois EJ, Camp JC, Farley DR, Fidler JL, Pawlina W, Robb RA. 2009: Virtual pelvic anatomy and surgery simulator: An innovative tool for teaching pelvic surgical anatomy. Stud Health Technol Inform 142:122-124.
Kraima AC, Smit NN, Jansma D, Wallner C, Bleys RLAW, Van De Velde CJH, Botha CP, Deruiter MC. 2013: Toward a highly-detailed 3D pelvic model: Approaching an ultra-specific level for surgical simulation and anatomical education. Clin Anat 26:333-338.
https://doi.org/10.1002/ca.22207
Miller R. 2000: Approaches to learning spatial relationships in gross anatomy: Perspective from wider principles of learning. Clin Anat 13:469-443.
https://doi.org/10.1002/1098-2353(2000)13:6<439::AID-CA8>3.0.CO;2-X
Nicholson DT, Chalk C, Funnell WR, Danial SJ. 2006: Can virtual reality improve anatomy education? A randomized controlled study of a computer-generated three-dimensional anatomic ear model. Med Educ 40:1081-1087.
https://doi.org/10.1111/j.1365-2929.2006.02611.x
Nygaard I, Barber MD, Burgio KL, Kenton K, Meikle S, Schaffer J, Spino C, Whitehead WE, Wu J, Brody DJ. 2008: Prevalence of symptomatic pelvic floor disorders in US women. JAMA 300(11):1311-1316.
https://doi.org/10.1001/jama.300.11.1311
Qayumi AK, Kurihara Y, Imai M, Pachev G, Seo H, Hoshino Y, Cheifetz R, Matsuura K, Momoi M, Saleem M, Lara-Guerra H, Miki Y, Kariya Y. 2004: Comparison of computer-assisted instruction (CAI) versus traditional textbook methods for training in abdominal examination (Japanese experience). Med Educ 38:1080-1088.
https://doi.org/10.1111/j.1365-2929.2004.01957.x
Raoof A, Henry RW, Reed RB. 2007: Silicone plastination of biological tissue: Room-temperature technique DowTM/Corcoran technique and products. J Int Soc Plastination 22:21-25.
https://doi.org/10.56507/AWAC9285
Sergovich A, Johnson M, Wilson TD. 2010: Explorable three-dimensional digital model of the female pelvis, pelvic contents, and perineum for anatomical education. Anat Sci Educ 3:127-133.
https://doi.org/10.1002/ase.135
Sora MC, Jilavu R, Matusz P. 2012: Computer aided three-dimensional reconstruction and modeling of the pelvis, by using plastinated cross sections, as a powerful tool for morphological investigations. Surg Radiol Anat 34:731-736.
https://doi.org/10.1007/s00276-011-0862-2
Sora MC, Jilavu R. 2013: Three dimensional reconstruction of a female pelvis using plastinated cross-sections - Using plastination for 3D reconstruction. J Plastination 25(1):22-27.
https://doi.org/10.56507/UFRG5276
Sugand K, Abrahams P, Khurana A. 2010: The anatomy of anatomy: A review for its modernization. Anat Sci Educ 3:83-93.
https://doi.org/10.1002/ase.139
von Hagens G. 1979a: Impregnation of soft biological specimens with thermosetting resins and elastomers. Anat Rec 194(2):247-255.
https://doi.org/10.1002/ar.1091940206
Von Hagens G. 1979b: Emulsifying resins for plastination. Der Praparator 25(2):43-50.
von Hagens G. 1986: Heidelberg Plastination Folder: Collection of technical leaflets for plastination. Biodur Products, Rathausstrasse 18, Heidelberg. 69126. pp 2:1-6, 3:1-13, 4:1-20, 5:1-17.
Wu Y, Zhang SX, Luo N, Qiu MG, Tan LW, Li QY, Liu GJ, Li K. 2010: Creation of the digital three-dimensional model of the prostate and its adjacent structures based on Chinese visible human. Surg Radiol Anat 32(7):629-635.
https://doi.org/10.1007/s00276-010-0625-5