Frauenklinik2 and Anatomisches Institut1 University of Heidelberg, 6900 Heidelberg 1, West Germany
Carcinomas of the female breast are judged to be mostly multicentric (Fisher et al., 1975; Gallager and Martin, 1969; Morgenstern et al., 1975) and only total breast removal was recommended until about 1960. Since then, breast conserving therapy (BCTh), i.e. surgical excision of the tumor in combination with radiotherapy of the remaining breast, has been performed in selected patients. The survival rate of BCTh patients is not significantly different when compared to total breast removal, and the local recurrence rate is about 4-8% in five years (Fisher and Wolmark, 1986; Veronesi et al., 1986). In 70-90% of local failures following BCTh, carcinoma growth was found at the primary tumor site. Four hypotheses may serve as possible reasons:
These questions may only be answered after complete histological examination of breasts from total mastectomy patients suited for BCTh.
Plastination; E12; Sheet Plastination
Gunther von Hagens Anatomisches Institut University of Heidelberg, 6900 Heidelberg 1, West Germany

![]()



Carcinomas of the female breast are judged to be mostly multicentric (Fisher et al., 1975; Gallager and Martin, 1969; Morgenstern et al., 1975) and only total breast removal was recommended until about 1960. Since then, breast conserving therapy (BCTh), i.e. surgical excision of the tumor in combination with radiotherapy of the remaining breast, has been performed in selected patients. The survival rate of BCTh patients is not significantly different when compared to total breast removal, and the local recurrence rate is about 4-8% in five years (Fisher and Wolmark, 1986; Veronesi et al., 1986). In 70-90% of local failures following BCTh, carcinoma growth was found at the primary tumor site. Four hypotheses may serve as possible reasons:
These questions may only be answered after complete histological examination of breasts from total mastectomy patients suited for BCTh.
Guhr and co-workers (1987) described sheet plastination as the best method for fast, complete histological study of mastectomy specimens. In the present study using sheet plastination, frequency and topographical distribution of tumor foci, which remain in the breast after BCTh, were evaluated in 131 patients.
Between 1978 and 1981, modified radical mastectomies with full axillary dissections were carried out for invasive carcinomas in 695 patients at the Division of Gynecology and Obstetrics, University of Heidelberg. From this group, 131 cases were selected which fulfilled our criteria for breast conserving therapy. These criteria were as fol1ows:
Histological examination, as described by Guhr and co-workers (1987), was utilized on the formalin- fixed specimens. Specimens were cut into 2.5 mm thick slices, stained with hematoxylin (Wellings and Jensen, 1973), and completely impregnated with a curable clear epoxy and cured (von Hagens, 1979). By focusing the microscope through the full thickness of the slice, microscopic evaluation through the entire thickness (2.5µ) of the slices was possible at magnifications up to 100X (Figs, la, 2a). A three-dimensional picture of relevant alterations was possible by viewing adjacent slices. Suspect areas were cut out from the large plastinated section and glued on wooden blocks; from which 5µ plastic sections were prepared, re-stained with hematoxylin-eosin and examined microscopically (Figs, 1b, 2b).
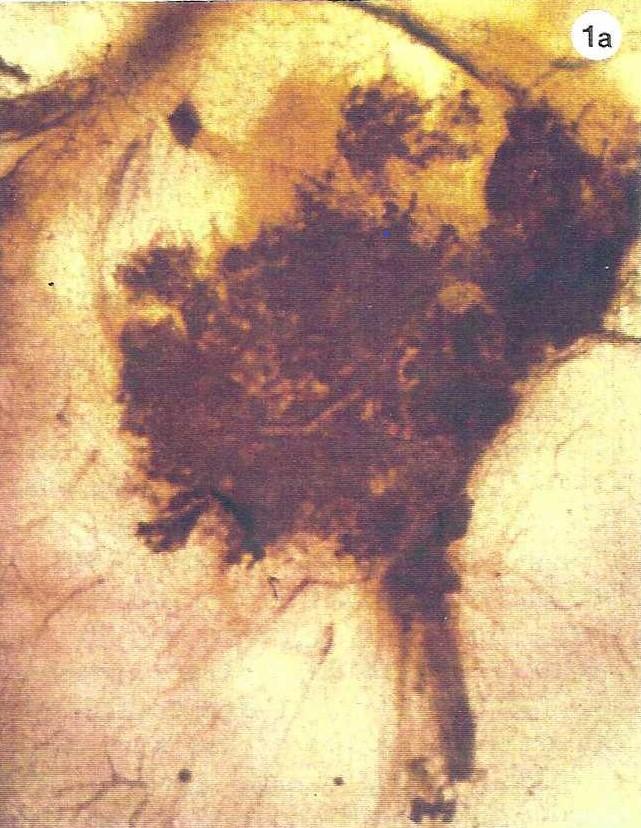 Figure la. Photomicrograph of a 2.5 mm thick plastinated breast tissue slice with adenosis. 25X. |
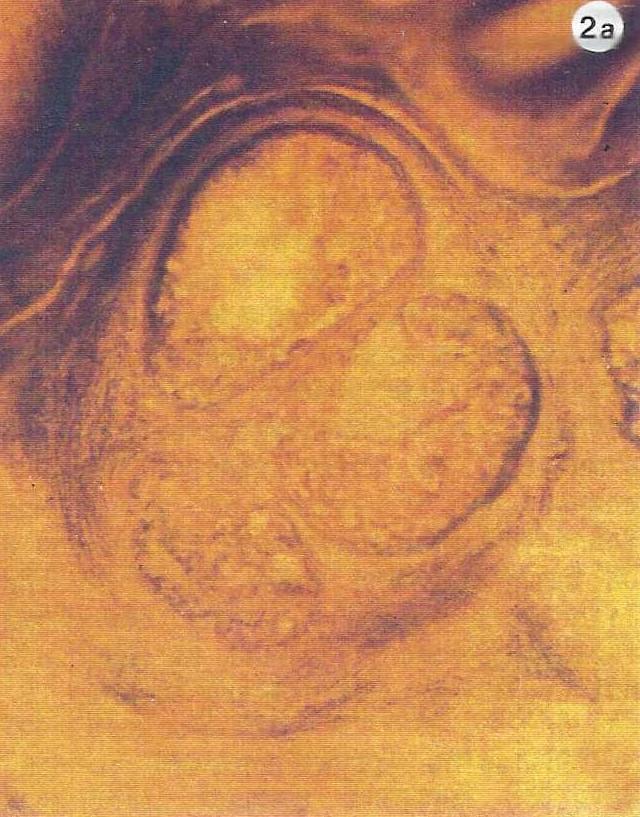 Figure 2a. Photomicrograph of a 2.5 mm thick plastinated breast tissue slice. The diagnosis is unclear, proliferative mastopathy with atypical epithelium or noninvasive ductal carcinoma. 25X. |
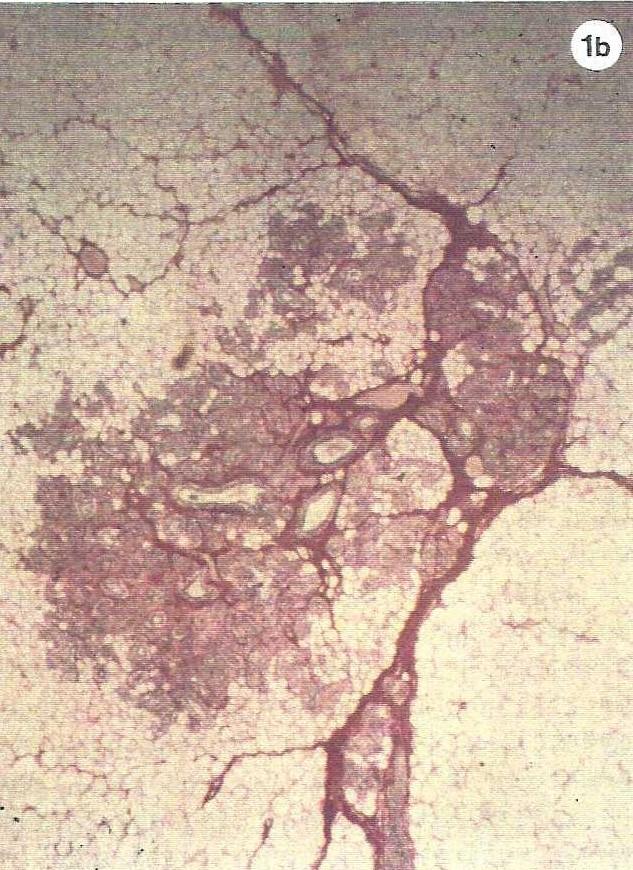 Figure lb. Histological section (5Μ) of the plastinated slice in figure la, used to confirm diagnosis. Hematoxylin eosin stain. 25X. |
 Figure 2b. Histological section (5µ) from the suspect region in Figure 2a used to diagnose ductal carcinoma in situ. Hematoxylin eosin stain. 100X. |
Carcinomas found in the specimen were recorded in topographic charts, thus showing their distribution pattern (Fig. 3). Quadrantectomies were simulated within these charts. From these topographic charts, "multicentric" tumor foci were those carcinomas which lay outside of the quadrants and had no connection to the primary tumor. Carcinomas, which were present outside the simulated resection area and had a connection to the primary tumor, were defined as "residuals of the primary tumor". If two invasive tumors were connected by a noninvasive ductal carcinoma which was present in all slices and throughout the entire thickness of the slices, a connection was considered to exist.
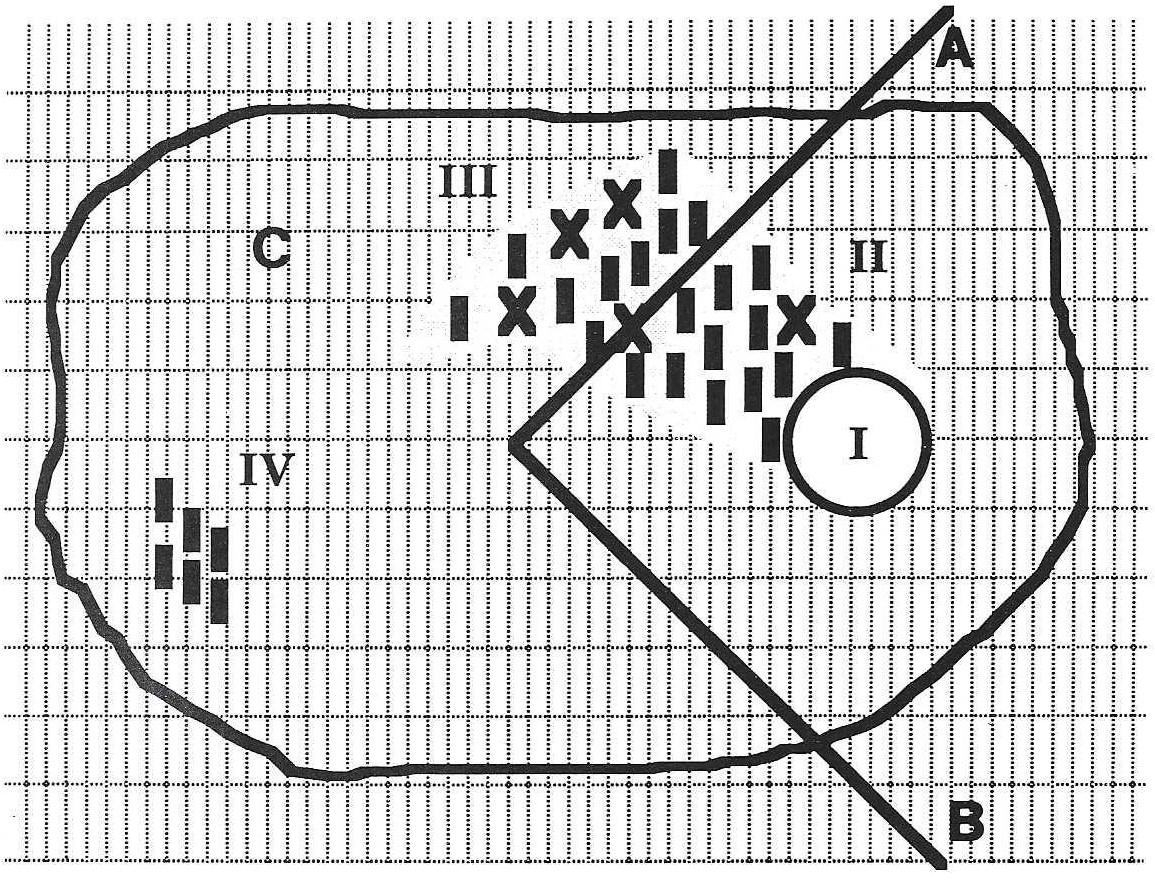 Figure 3. Topographical chart of a mastectomy specimen. After simulated quadrantectomy, extensions (II) of the primary tumor (I) extend to the resection line, while residuals (III) of the primary tumor extend from the margin of resection and into the remaining breast. A multicentric tumor focus (IV), with partly invasive growth, is observed in the remaining tissue. X = invasive carcinoma, I = noninvasive carcinoma, A and B = resection line of simulated quadrantectomy, C = remaining breast after quadrantectomy, distance between vertical lines = 0.5 cm and between two horizontal lines =1.0 cm. |
Following simulated quadrant- ectomy, carcinomas were found in 42 cases (32%), of which 24 (57%) were invasive carcinomas. The remaining 18 cases (43%) were noninvasive. Evaluation of topographical charts revealed 15 cases with both residuals and multicentric foci.
Multicentric foci, without any connection to the primary tumor, were found in 24.4% of the cases (32/131). Of these 32 multicentric carcinomas, 13 (41%) had invasive growth. The remaining 19 multicentric carcinomas (59%) showed noninvasive growth. Residuals of the primary, in the vicinity of the resection line, were found in 19.1% (25/131) of the cases and 12 (48%) of these residuals displayed invasive growth. Thirteen of the 25 residuals (52%) did not show any invasion.
Following BCTh, 70-90% of local failures occur in the vicinity of the primary tumor (Fisher et al., 1986; Muller, 1989a; Schnitt et al., 1985). Therefore, the question arises "whether the high rate of multicentricity found in the literature of up to 70% (Gallager, 1969; Morgenstern, 1975) can be applied to patients selected for conservative carcinoma therapy". However, since information regarding the size of either the primary tumor or multicentricity prior to mastectomy is missing in most studies, applicability seems unlikely. Rosen and co-workers (1975), for example, provided mammographic pictures for only 50% of their cases. For this present study, only patients suited for BCTh (primary tumor < 3 cm, no preoperative indication of multi- centricity or bilateral carcinomatous growth, distance from tumor to areola > 2 cm) were used. Rather than using segmental resection as Muller et al. (1989b), "quadrantectomies" were simulated in this study. Thus a comparison of rates of carcinomas found in remaining breast tissue could be compared with rates found in the literature (usually termed carcinoma foci multicentric, found in quadrants not containing the primary tumor). Following quadrantectomy in our selected patient group, carcinomas were observed in 32% of these cases. This tumor rate corresponds with results of Rosen et al. (1975), Lesser et al. (1982), and Westman-Naeser et al. (1981) who used chronological patient selection and incomplete histological examination (two to three slices from quadrants not containing the primary tumor). This collection, following chronological hospital admission or surgery dates, includes patients who are, however, not suited for BCTh because of tumor diameter, tumor location, or multicentricity already diagnosed preoperatively.
In order to apply our results to patients actually having undergone breast conserving therapy, it was not only necessary to study a comparable group of patients, but to answer the question of whether carcinomas remaining in the breast following quadrantectomy were simply residuals of incompletely excised primaries, or in fact, multicentric tumors independent of the primaries. In practice, through close histological examination of resection lines of the excised quadrants, BCTh facilitates both diagnosis of incomplete excision of the tumor and planning appropriate therapy based upon these findings.
The necessary differentiation of carcinomas discovered following quad- rantectomy, between "residuals of the primary" and actual "independent multicentric foci", is possible only through histological examination of the entire breast.
To date, the literature presents two techniques for the evaluation of the complete breast. Lagios and co- workers (1981) and Egan (1982) lamellated specimens in 2.5 and 5 mm thick slices, respectively, which were then radiographed. The radiographs were examined using a magnifier and suspect tissue areas were selected for further histological evaluation. However, this was time consuming, taking one pathologist and two technicians five years to evaluate 161 breasts (Egan, 1982).
After staining with hematoxylin, Wei lings and co-workers (1973, 1975) impregnated 2 mm thick tissue slices with methyl salicylate. These trans- parent slices were sealed in plastic bags which contained a liquid medium, and then evaluated with a magnifier or a dissecting microscope at 2-4 X. Any suspect region was excised and examined histologically following paraffin impregnation. This procedure is also time consuming, six weeks were needed to evaluate one breast as 300-500 histological slices were prepared. The unpleasant odor of the methyl salicylates necessitates the sealing of tissue slices. With sheet plastination, a breast examination is complete within seven days.
In our study group, an average of 20-25 histological sections 5µ thick were prepared per breast. Compared to the Welling's technique, this lower number of histological slices most likely results from evaluation of the plastinated tissue slices under much higher magnification (up to 100X). In addition, the solid consistency of the plastinated serial slices allows effortless spatial reconstruction of any anatomical alteration.
Sheet plastination allows complete microscopic evaluation of the female breast within a short period of time for even large specimens like: quadrantectomy or subcutaneous mast- ectomy specimens. Evaluation of our plastinated mastectomy specimens revealed residuals of the primary tumor remaining in 19% of cases evaluated, even with primary tumor size < 3 cm and generous resection through quadrantectomy. This is therapeutically relevant, as these results suggest the necessity of careful histological examination of resection lines of resectates, with alteration of therapy according to the results of this examination. Even then, due to clinically occult multicentric tumor foci which may not be identifiable even by the best histological examinations of the margins of the resectates, irradiation of the entire breast must be suggested.
Egan RL: Multicentric breast carcinomas. Clinical-radiographic- pathologic whole organ studies and 10-year survival. Cancer 49:1123- 1130, 1982.
https://doi.org/10.1002/1097-0142(19820315)49:6<1123::AID-CNCR2820490610>3.0.CO;2-R
Fisher B, N Wolmark: Conservative surgery: The American Experience. Semin Oncol 13:425-433, 1986.
Fisher ER, RM Gregorio, C Redmond, F Vellios, SC Sommers, B Fisher: Pathologic findings from the National Surgical Adjuvant Breast Project (Protocol No. 4). I. Observations concerning the multicentricity of mammary cancer. Cancer 35:247-254, 1975.
https://doi.org/10.1002/1097-0142(197501)35:1<247::AID-CNCR2820350130>3.0.CO;2-S
Fisher ER, R Sass, B Fisher, R Gre- gorio, R Brown, L Wickerham: Path- ological findings from the National Surgical Adjuvant Breast Project (Protocol 6). II. Relationship of local recurrence to multicentri- city. Cancer 57:1717-1724, 1986.
https://doi.org/10.1002/1097-0142(19860501)57:9<1717::AID-CNCR2820570902>3.0.CO;2-H
Gallager HS, JE Martin: Study of mammary carcinoma by mammography and whole organ sectioning. Cancer 23:855-873, 1969.
https://doi.org/10.1002/1097-0142(196904)23:4<855::AID-CNCR2820230420>3.0.CO;2-8
Guhr A, A Miiller, HW Anton, G von Hagens, H Bickley: Complete exam- ination of specimens using sheet plastination with epoxy resin. J Int Soc Plastination 1:23-39, 1987.
https://doi.org/10.56507/NXYR1705
Holland R, SHJ Veling, M Mravunac, JHCL Hendriks: Histologic multi- focality of Tis, Tl-2 breast carcinoma. Indication for clinical trials of breast conserving surgery. Cancer 56:979-990, 1985.
https://doi.org/10.1002/1097-0142(19850901)56:5<979::AID-CNCR2820560502>3.0.CO;2-N
Lagios MD: Multicentricity of breast carcinoma demonstrated by routine correlated serial subcross and radiographic examination. Cancer 40:1726-1734, 1977.
https://doi.org/10.1002/1097-0142(197710)40:4<1726::AID-CNCR2820400449>3.0.CO;2-O
Lagios MD, PR Westdahl, MR Rose: The concept and implications of multi- centricity in breast carcinoma. Pathol Annu 16:83-102, 1981.
Lesser ML, PP Rosen, DW Kinne: Multicentricity and bilaterality in invasive breast carcinoma. Surg 91:234-240, 1982.
Morgenstern L, PA Kaufmann, NB Friedmann: The case against tylectomy for carcinoma of the breast. The factor of multi- centricity. Am J Surg 130:251-258, 1975.
https://doi.org/10.1016/0002-9610(75)90379-7
Muller A: Patho-anatomic charac- teristics of local treatment failure following breast conserving therapy. In: Breast Disease. Eds. F Kubli , D von Fourn ier . Springer, Heidelberg & Berlin, pp. 82-87. 1989a.
https://doi.org/10.1007/978-3-642-73523-3_30
Muller A, D von Fournier, M Kaufmann, HF Otto, U Abel: Whole breast irradiation and boost irradiation in breast conserving therapy depending on morphological findings. Breast Dis 2:, 1989b. (In press).
Rosen PP, AA Fracchia, JA Urban, D Schnitt SJ, JC Connolly, A Recht, B Silver, JR Harris: Breast relapse following primary radiation therapy for early breast cancer. II. Detection, pathologic features, and prognostic significance. Int J Radiat Oncol Biol Phys 11:1277- 1284, 1985.
https://doi.org/10.1016/0360-3016(85)90242-1
Veronesi U, A Banfi, M Vecchio, R Saccozzi, C Clemente, M Greco, A Luini, E Marubini, G Muscolino, F Rilke, V Sacchini, B Salvadori, A Zecchini, R Zucali: Comparison of Hal stead mastectomy with quadrantectomy, axillary dis- section, and radiotherapy in early breast cancer: Long-term results. Eur J Cancer Clin Oncol 22:1085- 1089, 1986. https://doi.org/10.1016/0277-5379(86)90011-8
von Hagens G: Impregnation of soft biological specimens with thermosetting resins and elastomers. Anat Rec 194:247-256, 1979. https://doi.org/10.1002/ar.1091940206
Wellings SR, HA Jensen: On the origin and progression of ductal carcinoma in the human breast. J Natl Cancer Inst 50:1111-1118, 1973. https://doi.org/10.1093/jnci/50.5.1111
Wellings SR, HM Jensen, RG Marcum: An atlas of subcross pathology of the human breast with special reference to possible precancerous lesions. J Natl Cancer Inst 55:237-273, 1975.
Westman-Naeser S, E Bentsen, 0 Erikson, T Jarkans, B Nordin, B Stenkvist: Multifocal breast carcinoma. Am J Surg 142:255-257, 1981. https://doi.org/10.1016/0002-9610(81)90288-9