Department of Medical Education, College of Medicine & Life Sciences, University of Toledo, Toledo, Ohio, USA
One of the most significant disadvantages of silicone plastination of brain tissue can be shrinkage. Sucrose has been used as a cryoprotectant prior to processing in many neuroscience techniques. Our previous experiments included evaluating the efficacy of sucrose treatment in protection of brain tissue during silicone plastination techniques. The results were deemed inconclusive due to the number of variables present in the experimental protocol. The purpose of this study was to reevaluate sucrose treatment of nervous system as a means of preventing shrinkage in a more controlled environment. In addition to sucrose, dimethyl sulfoxide (DMSO) was tested as a solvent media. The experimental groups follow: control (no treatment), sucrose treatment, and DMSO treatment. Care was taken to normalize all known variables to only produce variance in initial treatment prior to dehydration. Four brains fixed in 10 % formalin were sectioned coronally using a deli slicer to produce 1 cm thick slices (samples). Each slice was divided into right and left hemispheres. The right hemispheres were used as controls and the left hemispheres were used as the experimental groups. Therefore. each experimental sample could be compared to an equivalent control sample from the same region of the brain. Two brains were used in each experimental group. The experimental groups were immersed in 10% sucrose or DMSO, respectively at 5 degrees Celsius (overnight) prior to dehydration. The control group was immersed in distilled water at 5 degrees overnight prior to dehydration. For dehydration, the specimens were submerged in – 25º C cold acetone. After dehydration the specimens were submerged in - 15º C cold silicone impregnation-mix. After each step of plastination, pictures were taken and surface area was calculated of each slice/specimen using image analysis software (IMAGEJ, NIH). To determine the correlation between treatment and control, the average percent shrinkage was calculated for both experimental groups. Findings are summarized as follows: control group 38.5% shrinkage, sucrose treatment group 31.9% shrinkage, DMSO treatment group 39.4%. The sucrose treatment had the least shrinkage. Other notable findings include greatest shrinkage occurring during the curing step (32.5% sucrose-treated, 37.7% DMSO-treated). For brain 1 and brain 2, the difference between the DMSO - treated brain and the control was not statistically significant. For brain 3, there was a statistically significant difference between the sucrose-treated brain and the control as determined by one-way ANOVA (F (1,10) = 7.947, P = 0.018). Finally, for brain 4, there was a statistically significant difference between the sucrose-treated brain and the control as determined by one-way ANOVA (F (1,22) = 11.463, P = 0.003). Treating brain tissue with 10% sucrose prior to plastination is effective in decreasing shrinkage.
shrinkage, sucrose, brain, slices, silicone, cryoprotectant, DMSO
Carlos A. C. Baptista, Department of Medical Education, College of Medicine, University of Toledo, Toledo, Ohio USA 43614, Email: carlos.baptista@utoledo.edu

![]()



In the 1980s the advent of histochemistry for the study of the central nervous system required that tissue sections need to be prepared without embedding in paraffin, plastic, or celloidin, since these procedures reduce or abolish many forms of histochemical activity. An alternative for many studies was to freeze the specimen and to produce frozen sections on a cryostat. One problem that often occurred with this procedure was the appearance of large vacuoles in the tissues, presumably created by formation of ice crystals which displaced normal tissue. In order to protect the tissue from the ice crystal formation a cryoprotectant was used. Sucrose was the cryoprotectant of choice for most neuroanatomical techniques. The infiltrating of the tissue before freezing with a solution of 30% sucrose in buffer was advocated by many researchers (Rosene et al., 1986).
Another useful cryoprotectant agent used in neuroscience techniques is dimethyl sulfoxide (DMSO). One of the particularly attractive features of DMSO was its rapid and apparently universal penetration into cells (Meryman, 1971).
In Plastination, dehydration by freeze-substitution is based on a principle similar to cryosubstitution, a dehydration procedure used in histochemistry and electron microscopy. Tissue to be dehydrated is removed from the fixative and placed in -25°C acetone. Upon immersion in the acetone, water within the specimen freezes immediately, providing an internal framework for dimensional stability. Slow substitution of ice by acetone then results in only minor shrinkage.
The purpose of this study is to determine whether sucrose treatment is an effective means of preventing shrinkage in the silicone plastination technique of brain tissue. No systematic studies that demonstrate sucrose’s crypoprotective usefulness in dehydration of brain tissue for plastination were found in the literature review.
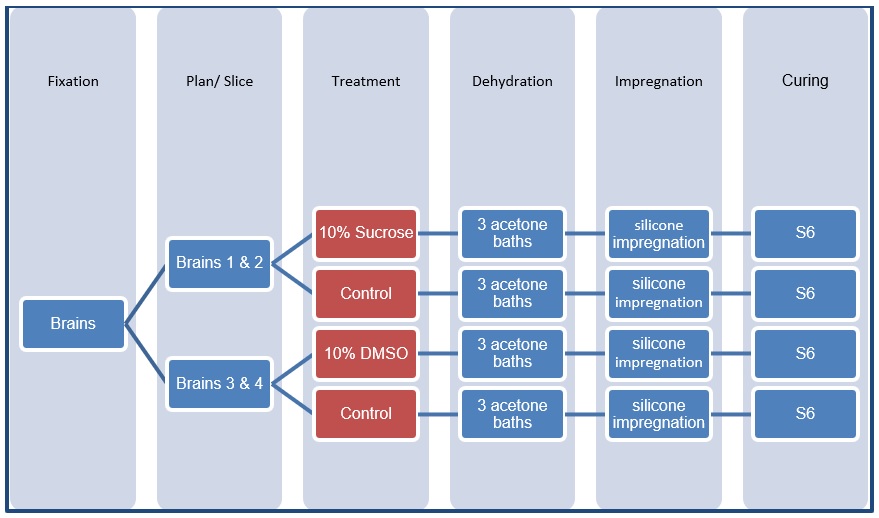 Figure 1: The experimental design to test the effects of sucrose and DMSO on brain shrinkage. |
The four basic steps of silicone plastination follow: fixation and preparation, dehydration, impregnation, and curing. In order to test for the effects of a cryoprotectant in preventing shrinkage, the specimens were immersed in sucrose or DMSO before dehydration. The experimental design is illustrated in Figure 1.
Specimen Preparation
Fixation: Four human brains fixed in 10% formalin were used for this experiment. Each brain had a different fixation time: 13 months, 14 months, 15 months, and 16 months old. The brains were chosen randomly from a collection of fixed brains. It is our experience that using brains fixed for a minimum of 4 to 6 months is ideal for plastination
Preparing and Slicing Brain: Each whole brain was sectioned using a deli slicer producing 10 mm thick coronal slices (“specimens”). Each slice was divided into right and left hemispheres. The right hemispheres were used as control groups and the left hemispheres were divided into experimental groups. Therefore, each experimental specimen could be compared to specimens from the opposite side of the same region of the brain.
Flushing and Precooling: The specimens were washed in cold, running tap water overnight to remove most of the formalin. In the process, the specimens were cooled to 5 ºC in preparation for dehydration and were photographed.
Immersion in sucrose or DMSO: Two brains were used in each experimental group. Each experimental group was immersed in either 10% sucrose or 10% DMSO at 5º C overnight prior to dehydration. The control group was immersed in distilled water at 5º C overnight prior to dehydration and were photographed.
Dehydration
Dehydration of the specimens was performed using freeze substitution in -25º C acetone (von Hagens, 1986, Henry et al., 2019). The acetone was pre-cooled to -25° C in the deep freezer and divided into three containers designated according to treatment solvent: control, sucrose, and DMSO. Before all specimens were placed in the respective labeled containers of acetone, acetone purity was measured with an acetonometer. Specimens were submerged in one of the three baths of 100% acetone. The specimens were held in the first bath of 100% acetone (in the freezer) to dehydrate for three days, at which point the acetone in the containers was agitated to allow the settled water to mix with the acetone. An aliquot of the used acetone was brought to room temperature (20º C). The specific gravity of the acetone (purity) was measured with an acetonometer calibrated at 20º C. The specimens were transferred to the second bath of pure (100%), pre-cooled (-25 ºC) acetone. Again, after three days the acetone bath was agitated, and the purity was measured as before. A third acetone bath followed the same procedure as the second acetone bath. Acetone concentration was monitored with an acetonometer to determine the purity of the acetone after each bath. Dehydration was considered complete when acetone purity was 99% or greater. There were three acetone changes for each brain and post dehydration pictures were taken.
Forced Impregnation
The impregnation chamber was prepared with the pre-cooled silicone impregnation-mixture (NCS10/3). The specimens were transferred quickly from the acetone to the silicone impregnation-mixture and submerged in the mixture over night. A grid was used to keep the specimens submerged in the resin. The following morning the vacuum pump was turned on. The pressure in the vacuum chamber was slowly lowered over the course of several days. Each day of impregnation, the impregnation bath was checked for bubbles. The visibility of small bubbles indicates acetone vaporization out of the specimens and its replacement with silicone resin. The pressure was lowered only when bubbles were no longer visible on the surface of the polymer. The maximum vacuum achieved was 1-2 mmHg. The vacuum pump was shut off, and the specimens remained in the sealed chamber overnight. Next day, the specimens were removed from the chamber and let drain inside the deep freezer. When no excess resin was seen oozing from the specimens, the set of slices was allowed to drain at room temperature. At this time, the specimens were prepared for curing (DeJong and Henry, 2007). Photographs were taken for surface area measurements.
Gas Curing/ Hardening
Before curing, the specimens were fully drained and blotted dry at room temperature. The specimens were exposed to S6 vapors for three days, or until the desired hardness was achieved. The specimens were flipped halfway through the curing process to allow completion. After gas curing, when the specimens were hard and dry, the specimens were photographed placed in sealed plastic bags to allow further internal hardening.
Data Collection
The brain slices were photographed using a Kodak MXY camera after each step of the process (after slicing; after dehydration; after impregnation; after curing). The images were downloaded to a computer and processed through ImageJ software. Each photograph contained a controlled size grid (1 millimeter) to permit calibration of the software during measurement. After calibration, changes in surface area were tracked by recording the brain images at each step. The first set of images were acquired after slicing/washing the specimens prior to immersing into media (DMSO or sucrose) and used as the initial measurement before any shrinkage had occurred. Successive data collection occurred after dehydration, impregnation, and curing. Caution was taken to prevent specimens from warming to room temperature during the data collection process. The specimens were kept at –25°C with the help of ice baths except for when the picture was taken. However, this was done through a highly efficient process which minimally exposed the sample. The surface areas of the specimens were measured after each step of plastination using image analysis software (IMAGEJ, NIH). Each measurement was repeated three times for each specimen and the average surface area was used as the final measurement.
Seventy-six brain slices were prepared for and successfully plastinated. Pictures were taken at prescribed stages throughout the process which were used to calculate the area of the treated slices and compare with the area of the control slice of the same region. They were divided as follows: 19 (sucrose treated), 19 (control/sucrose group), 19 (DMSO treated), 19 (control/DMSO group).
The average percent shrinkage of the brain slices was calculated for each experimental group using the control of that group.
Findings are summarized in the figures and are as follows: control group (no treatment) 38.7% shrinkage, sucrose-treated group 31.9% shrinkage, DMSO-treated group 39.4% and DMSO control group 38.2%. The sucrose treated group resulted in the least overall shrinkage (figure 2). The shrinkage comparison between sucrose-treated and control group is displayed in figure 3. The shrinkage comparison between DMSO-treated and control group is displayed in figure 5. A comparison was made between surface area variation of sucrose treated and sucrose control groups after specified steps of the plastination process, that is, after dehydration, impregnation, and curing (figure 4). A comparison was made between surface area variations of DMSO treated and DMSO control groups after specified steps of the plastination process, that is, after dehydration, impregnation, and curing (figure 6). The greatest area variation occurred during the curing step.
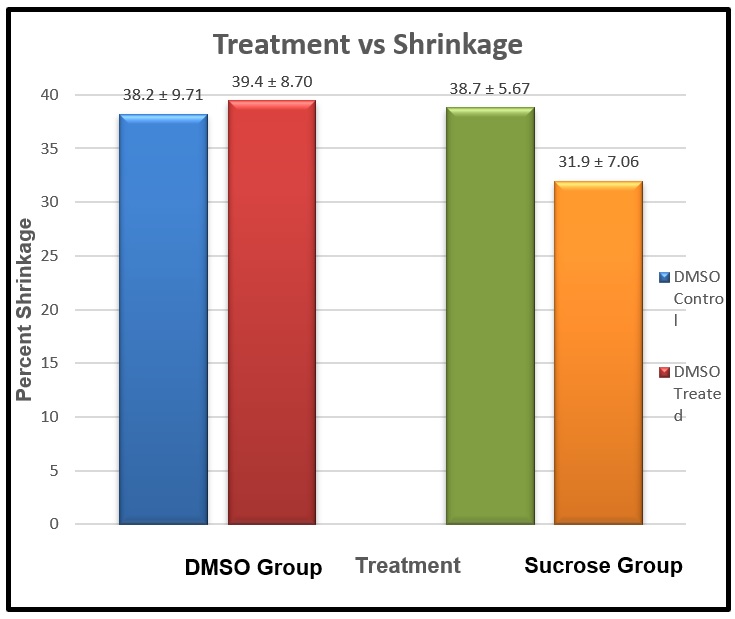 Figure 2: Percentage of total shrinkage at the end of the plastination process for the specimens treated with sucrose and DMSO and compared with appropriate controls. |
 Figure 3: Percentage of shrinkage in the sucrose-treated group |
|
 Figure 4: Percentage of surface area variation of the sucrose group after dehydration, impregnation, and curing phases of plastination. Initial measurement referred to after slicing/washing the specimen. |
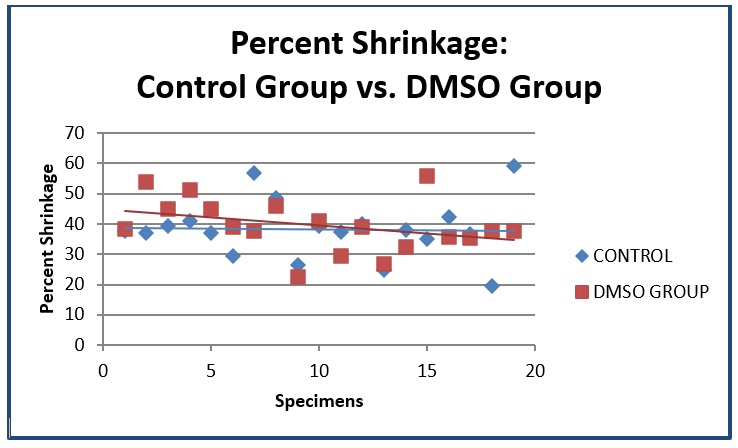 Figure 5: Percentage of shrinkage in the DMSO-treated group |
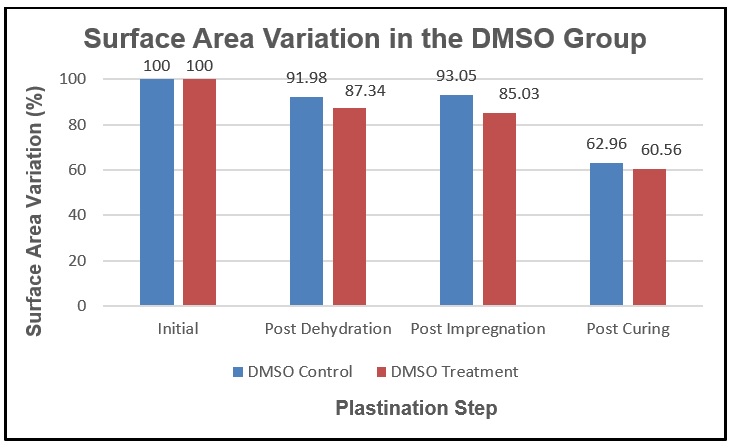 Figure 6: Percentage of surface area variation of the DMSO group after dehydration, impregnation, and curing phases of plastination. Initial measurement referred to after slicing/washing the specimen. |
Statistical Analysis: For brain 1 (DMSO-treated) and brain 2 (DMSO-treated), the difference between the DMSO-treated brain and the control was not statistically significant. For brain 3 (sucrose-treated), there was a statistically significant difference between the sucrose-treated brain and the control (no treatment) as determined by one-way ANOVA (F (1,10) = 7.947, P = 0.018). For brain 4 (sucrose-treated), there was a statistically significant difference between the sucrose-treated brain and the control as determined by one-way ANOVA (F (1,22) = 11.463, P = 0.003).
When designing the experiment, slices were obtained from four different brains with varying fixation lengths: 13 months, 14 months, 15 months, and 16 months. The brains were chosen randomly from a collection of fixed brains. It is our experience that using brains fixed for a minimum of 4 to 6 months is ideal for plastination. Using brains with less than the minimum time of fixation can result in excessive shrinkage. Fixation alters the cells on a molecular level increasing their mechanical strength or stability. The increased strength is translated by specimen rigidity therefore, preserving the morphology (shape and structure) of the brain. In order to evaluate the treatment of the brain in comparison with a control, we used one half-hemisphere of each brain as a control for that group. By doing this the different age of fixation would not interfere with the results since the control and experimental group came from the same brain.
Each individual brain slice was obtained from a different slice of the brain. Each slice had a different ratio of gray-to-white matter. Gray matter has a greater water composition (82%) in comparison to the composition of water in the white matter (72%), causing greater shrinkage in gray matter (Suzuki 1981; Suriyaprapadilok and Withyachumnarnkul, 1997). We considered this occurrence insignificant to our experiments since the white and gray matter were uniformly distributed among the different groups of brain tissue.
Dehydration using acetone freeze substitution is the gold-standard to dehydrate specimens for plastination, especially brain tissue. One of the possible complications that appeared using this technique is ice-crystal formation (von Hagens, 1986). Abnormal vacuoles in the tissues, is presumably created by the formation of large ice crystals, which displaced normal tissue. Crystal formation will distort microscopic morphology if the specimen is larger than 2 mm. (Tiedemann and Ivic-Matijas, 1988). Von Hagens 1986, recommend precooling the specimens to +5º C before start dehydration. Another solution to this problem is to protect the tissue from ice crystal formation by using a cryoprotectant.
Sucrose serves as a cryoprotectant by functioning as a partial dehydrant (Rosene et al., 1986), thus preventing the formation of ice crystals. Cryoprotectants serve as anti-freeze substances (ice-blockers) that hold the molecules in place rather than inducing crystallization (Rosene et al., 1986). Sucrose theoretically should serve as an efficient cryoprotectant in plastination. In our experiments, the use of sucrose proved to be beneficial because the shrinkage found in the specimens was significantly less than the control non-treated specimens. The same cannot be said regarding DMSO. The specimens treated with DMSO presented more shrinkage than the control non-treated specimens. We believe that the DMSO contained in the brain tissue cannot be as easily removed by the acetone, thus, competing as an inefficient intermediate solvent for silicone. The vapor pressure of DMSO is 0.600 mm Hg at 25º C, and freezing point is 18.55º C. DMSO has high dynamic viscosity (1.996sP). It is almost two times higher than the dynamic viscosity of 10% aqueous sucrose solutions (1.130sP). DMSO is also a polar solvent and does not mix well with the silicone polymer, preventing its penetration into the specimens. That would explains the higher shrinkage of the samples when DMSO is used as a cryoprotectant.
A statistical relationship was ascertained between sucrose-treated brain tissue shrinkage and the control (non-treated) brain. This may be a result of several factors that affected the quality of the plastinated specimen. When discussing shrinkage of brain tissue, many variables are relevant including: fixation time, ratio of gray-to-white matter of sample, length of impregnation, effect of cryoprotectants, freezing and rewarming specimens, and osmotic effects. In order to prevent shrinkage and maintain cell membrane integrity in our experiments, the diffusion rates of substances leaving and entering the cells must be equal. Shrinkage will occur in the following scenarios: water leaves at a faster rate than acetone enters the cell/intercellular space during dehydration or acetone diffuses out of the cell/intercellular space at a faster rate than silicone enters during impregnation. In our experiments it is possible to speculate that the rate of silicone entering the cell/intercellular space during the impregnation had an impact on the curing of the specimen. If during impregnation, acetone would leave the specimen but would not be completely replaced by polymer, the result would be empty cell/intercellular space. Therefore, during curing, cell structure would collapse so in consequence the specimen would shrink. The amount of shrinkage would depend on the amount of incomplete impregnation. One aspect of the impregnation that should be considered is the viscosity of the polymer and the temperature of impregnation. If the vacuum of 1-2 mmHg is reached and the polymer viscosity is high, impregnation can also be incomplete resulting in shrinkage. Increasing the temperature of impregnation will change the viscosity of the polymer and in consequence facilitates impregnation.
In conclusion, treating brain tissue with 10% sucrose is beneficial to reduce shrinkage.
Acknowledgements
The authors sincerely thank those who donated their bodies to science so that anatomical research could be performed. Results from such research can potentially increase mankind’s overall knowledge that can then improve patient care. Therefore, these donors and their families deserve our highest gratitude. Our special thanks to Dianne Durliat , Elizabeth Dalzel and the Anatomical Donation Program of the College of Medicine of the University of Toledo.
DeJong K, Henry RW. 2007: Plastination of biological tissue: Cold-temperature technique. J Int Soc Plastination 22:2-14
https://doi.org/10.56507/ZLMJ7068
Henry, R.W.; von Hagens, G; Seamans, G. 2019: Cold Temperature/Biodur/S10/ von Hagens'- Silicone Plastination Technique.Anat Histol Embriol: (48): 532-538.
https://doi.org/10.1111/ahe.12472
Klaus Tiedemann and Dubravka Ivic-Matijas 1988: Dehydration of Macroscopic Specimens by Freeze Substitution in Acetone. J. Int. Soc. Plastination 2 (2) : 2-12.
https://doi.org/10.56507/SCLL2742
Meryman HT 1971: Cryoprotective agents. Cryobiology 8:173.
https://doi.org/10.1016/0011-2240(71)90024-1
Rosene, D. L.; Roy, N, J.; Davis D, B. J. 1986: A Cryoprotection Method That Facilitates Cutting Frozen Sections of Whole Monkey Brains for Histological and Histochemical Processing Without Freezing Artifact. The Journal of Histochemistry and Cytochemistry 34(10): 1301-1315.
https://doi.org/10.1177/34.10.3745909
Suriyaprapadilok L, Withyachumnarnkul B. 1997: Plastination of stained sections of the human brain: Comparison between different staining methods. J Int Soc Plastination 12: 27-32.
https://doi.org/10.56507/YISQ6047
Suzuki, K. 1981: Chemistry and Metabolism of Brain Lipids. In: Basic Neurochemistry. Edited by Siegel GJ, Alters RW, Agranoff BW and Katzman R. 3rd., Boston: Ed. Little Brown and Company, pp 355-370.
Von Hagens G. Heidelberg Plastination Folder 1986: Collection of All Technical Leaflets for Plastination, Anatomisches Institut I Universitat Heidelberg, 2nd English Edition.