Department of Animal Science, The University of Tennessee, College of Veterinary Medicine, Knoxville, TN, 37901-1071, USA
Preparation of anatomically precise tracheobronchial casts with accompanying pulmonary arteries and/or veins are valuable teaching aids. To see the actual replica of the airway and the pulmonary vasculature, clarifies many questions in the student's mind. McLaughlin and co-workers (1961) made similar casts from vinylite and latex which are not as durable as silicone casts. The manufacturers of the various polymers are numerous, while the properties of these polymers are diverse. Charts are available which list the properties of many of the available polymers, thus generic polymers with similar properties can be purchased. Four polymers were used to make tracheobronchial casts with accompanying casts of the pulmonary vasculature.
vascular cast; bronchial cast; silicone
Robert W. Henry Department of Animal Science, The University of Tennessee, College of Veterinary Medicine, Knoxville, TN, 37901-1071, USA

![]()



Preparation of anatomically precise tracheobronchial casts with accompanying pulmonary arteries and/or veins are valuable teaching aids. To see the actual replica of the airway and the pulmonary vasculature, clarifies many questions in the student's mind. McLaughlin and co-workers (1961) made similar casts from vinylite and latex which are not as durable as silicone casts. The manufacturers of the various polymers are numerous, while the properties of these polymers are diverse. Charts are available which list the properties of many of the available polymers, thus generic polymers with similar properties can be purchased. Four polymers were used to make tracheobronchial casts with accompanying casts of the pulmonary vasculature.
Two silicone polymers were used to inject the pulmonary vasculature of eight lungs (4 each).
All components were combined and mixed using the manufacturer's recommendations. Biodur polymer ratio was 1:100 (S3:S10) but S2 was varied from 0.5:100 to 1.5:100 (in 0.5 increments). Since Biodur polymer is transparent, either red or blue color additive [Biodur color paste: AC 50 (red) or AC 52 (blue)] was used to give a color to the vessels. The red Rhone-Poulenc polymer was used as it came from the manufacturer, while the clear was tinted. Rhone-Poulenc hardener/polymer ratio was 1:10. Approximate quantity of polymer used per vascular cast was .2 - .5 kg (20 to 50 cc) / 20 kg dog, 1-2 kg (120 - 200 cc) for adult pig, ox or horse. For the airway casts, either the Rhone-Poulenc polymer # 1556 (clear) or the Dow Corning polymer-Silastic E RTV (white) [Dow Corning Corp., Midland, Ml 48640-0994, USA] was used.
Fresh dog, pig and ox lungs were procured from the necropsy area and from local abattoirs. The lungs were cannulated and flushed several time to remove the excess blood and secretions (Henry and Butler, 1990). The pericardium was removed from the heart. For a cast of the airway and pulmonary arteries, the majority of the heart was removed leaving the pulmonary trunk and aorta in situ. A cannula was ligated in place in the pulmonary trunk in preparation for injection of the polymer. The appropriate polymer (Rhone-Poulenc or Biodur) was mixed, tinted, drawn into 60 cc catheter tip syringes, and injected into the pulmonary arteries via the cannula in the pulmonary trunk. Injection proceeded until the color could be seen near the lung surface or until the resistance was notably increased. To aid visualization of filling, a small tear was made in the edge of a lung lobe. When polymer appeared at the tear, injection was ceased. For a cast of the pulmonary arteries and veins, a cannula was inserted through the aorta, past the aortic valves, through the left ventricle and A-V (mitral, bicuspid) valve, into the left atrium and ligated at the aorta. The right ventricle (conus arteriosus portion) was opened and a cannula inserted into and ligated in the pulmonary trunk. The selected polymer (Rhone-Poulenc or Biodur) was mixed, tinted, placed into 60 cc catheter tip syringes, and injected into the pulmonary arteries via the cannula in the pulmonary trunk or the pulmonary veins via the cannula in the aorta. Injection proceeded until the colored polymer could be seen near the lung surface or perimeter or until the resistance was notably increased. After the vessel injection was complete, the esophagus and any other mediastinal tissue and fat were removed from the lungs and tracheobronchial tree similar to McKiernan and Kneller (1983). The lungs were inflated and dried using compressed laboratory air directed into the trachea. Lungs were placed on their dorsal (posterior) surface on a tray to contain the extravasated fluid. The air flow was gradually increased until the lungs were inflated and remained inflated to near capacity. Air flow and inflation level were maintained until the lungs were thoroughly dried. After drying was complete, a selected polymer (Rhone-Poulenc or Dow Corning) was mixed, using the manufacturer's recommended ratio (1:10), and was poured into the trachea aided by an appropriate sized funnel. The quantity of polymer used per airway was .2 to .5 kg/ 20 kg dog, 1-2 kg for adult pig, horse or ox. In larger specimens before the silicone hardened, a heavy galvanized wire was placed into the lumen of the trachea to give support to the silicone cast. The polymer mixes were allowed to harden over night. The next morning, the lung unit was placed in a vat of simmering to slowly boiling water for several hours. The specimens were checked in four to five hours to determine if most of the lung and airway tissue had been macerated away from the cast material. Occasionally, at this time, a ligature was placed around the right and left primary bronchi and the associated vasculature of the casts. Following maceration, the cast was removed from the hot water and sprayed with a high pressure hose to remove remaining tissue. If tissue still remained, the cast was submerged either in hot water or in a 10% sodium hydroxide solution until the remaining tissue was released. The specimens were rinsed with water and allowed to dry before use.
Both polymers produced representative casts of the airways and pulmonary vasculature. More viscous polymers did not flow into the finest bronchi, alveoli and vessels (Fig. 1). The less viscous polymers flowed freely into the capillary bed and the small arteries ( Fig. 2). The Biodur polymer consistently was the least viscous and entered the smallest vessels (Fig. 3). Ratios of 1.5:100 of Biodur S2 usually hardened to quickly to fill the capillary bed while casts of 0.5:100 ratios remained tacky.
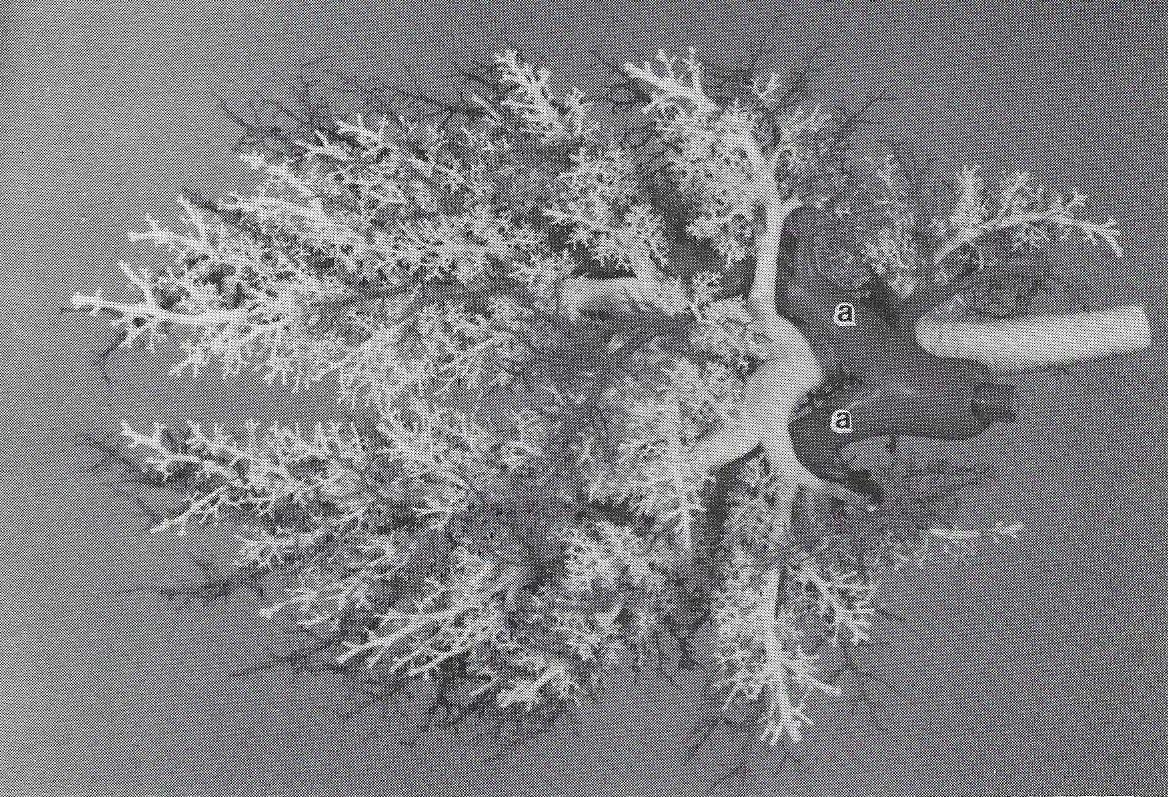 Figure 1. Tracheobronchial-vascular cast from an ox. Airways of Silastic E RTV and the arteries (a) of Rhone- Poulenc mixture (10:1). Note only the larger airways and arteries are filled. |
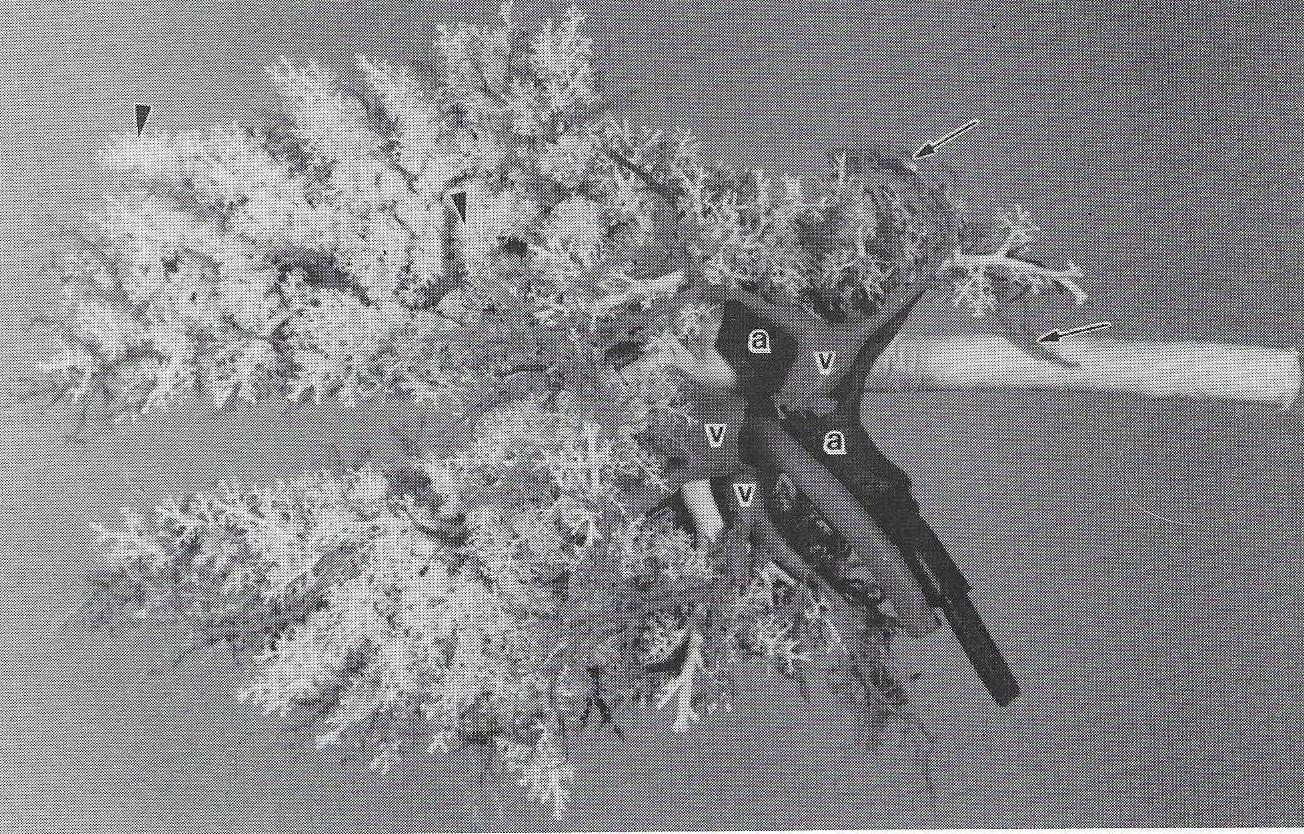 Figure 2. Tracheobronchial-vascular cast from a pig. Airways of Silastic E RTV and the arteries (a) and veins (v) of Rhone-Poulenc mixture (10:1). Note both large and small airways (arrowhead) are filled. Also, the polymer reached the smaller venules (arrow) and small arteries. |
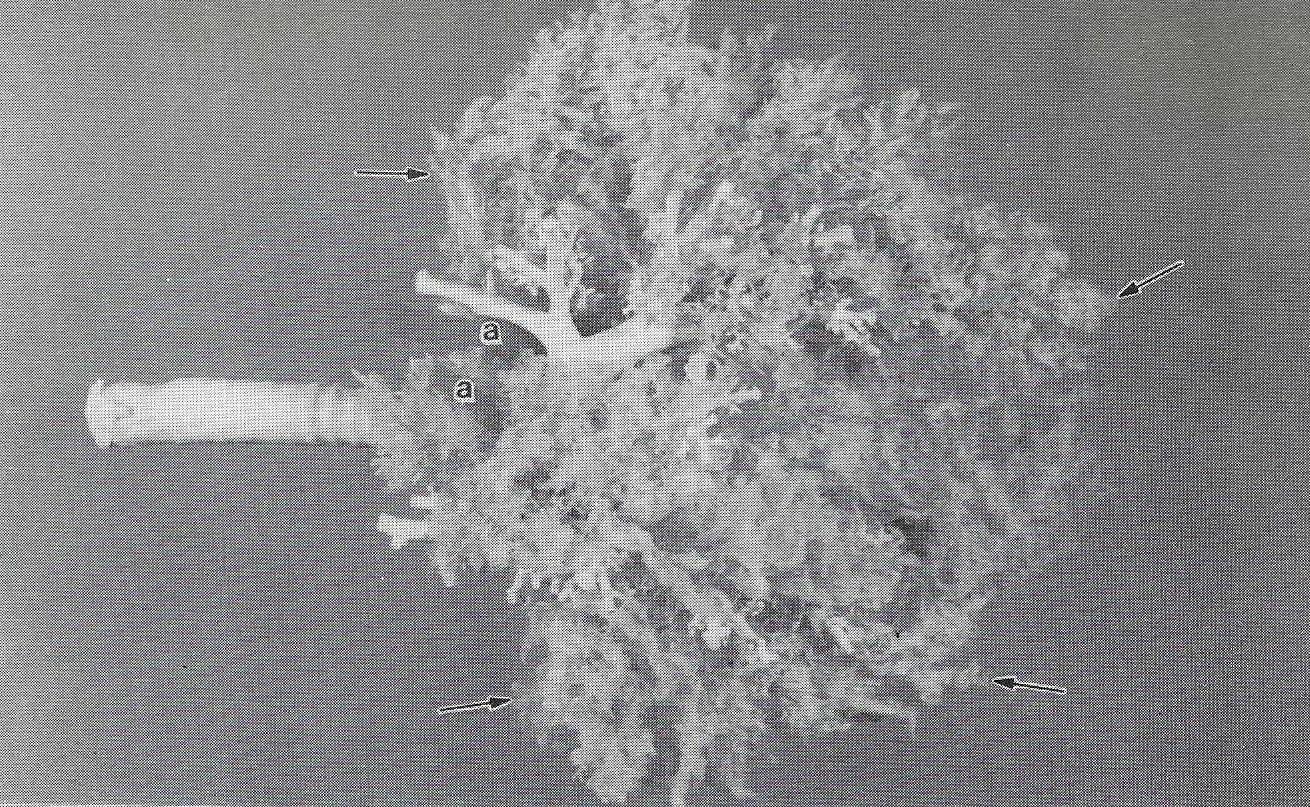 Figure 3. Tracheobronchial-vascular cast from a dog. Airways of Silastic E RTV and the arteries (a) of Biodur S10/S3/S2 mixture (100:1:1). Note only the larger airways are filled, however, the capillary bed (arrow) is complete. |
|
Representative casts of the airways with their pulmonary vasculature were produced with the selected polymers. The desired cast type must be determined before production. Low viscosity polymers flow freely into the alveoli and fill the entire airway and vessel. Whereas, more viscous polymer mixtures, due to less polymer entering the distal airways and vessels, present a more clear branching pattern. The optimal polymer hardener ratio for the Biodur product was 100:1:1. Viscosity of a polymer mixture may be increased by increasing the time interval between combining the polymer and hardener and actually pouring the mixture into the lungs or by increasing the quantity of hardener. Excess hardener will cause the mixture to set up rapidly and be difficult to flow into the smaller airways and vessels. Therefore, filling of the smaller vessels can be decreased or eliminated by waiting a few minutes before filling the vessels. Thus a cast may be produced which allows better visualization of whatever structures are desired. Securing the components of the cast with a string or wire helped keep the vascular components of the cast in proper orientation to the airways. When filling the pulmonary venous system, if the cannula is in the left ventricle instead of the left atrium, the A-V valve may close and not allow the veins to fill. However, this will produce a nice cast of the left ventricle, aorta and coronary vessels. Polymer cost is similar, $35.00/kg.
ACKNOWLEDGMENTS
A special thanks to Kreis Weigel and Dr. M. McCracken for help with the photography. Thank you to Emily Smathers for assistance with casting.
Henry RW, J Butler: Room-temperature "forced air" impregnation of dried lungs with S10/S3-xylene mix. J Int Soc Plastination 4:14-15,23, 1990.
https://doi.org/10.56507/KTGZ7837
Mckiernan BC, SK Kneller: A simple method for the preparation of inflated air-dried specimens. Vet Rad 24(2):58-62, 1983.
https://doi.org/10.1111/j.1740-8261.1983.tb01539.x
Mclaughlin RF, WS Tyler, RO Canada: A study of the subgross pulmonary anatomy in various mammals. Am J Anat 108:149-165, 1961.
https://doi.org/10.1002/aja.1001080203