Department of Animal Science, The University of Tennessee, College of Veterinary Medicine, Knoxville, TN, 37901-1071, USA.
Preparation of beautiful and anatomically precise tracheobronchial casts have an inherent teaching value. To actually see the replica of the airway instead of merely hearing a description of it or only seeing a figure rendered by an artist is an invaluable teaching aid. In addition to education, casts have been used for morphometric studies (Weibel and Gomez, 1962; Horsefield and Gumming, 1968; Pump, 1969). Some previously used resins produce brittle specimens which often shatter and may be totally destroyed if dropped (Tucker and Krementz, 1957). Frank and Yoder (1966) introduced the use of silicone for forming casts. Kilpper and Stidd (1973) devised a complicated method for filling the airways in a wet state to prevent shrinkage artifact, while Phalen and coworkers (1973) introduced making silicone casts of the airways in situ. We have chosen to use air-dried lungs, similar to Wang and Kraman (1988), to produce the casts. There are several manufacturers of polymer and numerous polymers to chose from. The properties of the polymers are just as diverse. Comparisons of the properties of polymers from the various manufacturers are available but not totally accurate. Five polymers of varying properties were used to make tracheobronchial casts.
Casts; Silicone; Biodur
Robert W. Henry Department of Animal Science, The University of Tennessee, College of Veterinary Medicine, Knoxville, TN, 37901-1071, USA.

![]()



Preparation of beautiful and anatomically precise tracheobronchial casts have an inherent teaching value. To actually see the replica of the airway instead of merely hearing a description of it or only seeing a figure rendered by an artist is an invaluable teaching aid. In addition to education, casts have been used for morphometric studies (Weibel and Gomez, 1962; Horsefield and Gumming, 1968; Pump, 1969). Some previously used resins produce brittle specimens which often shatter and may be totally destroyed if dropped (Tucker and Krementz, 1957). Frank and Yoder (1966) introduced the use of silicone for forming casts. Kilpper and Stidd (1973) devised a complicated method for filling the airways in a wet state to prevent shrinkage artifact, while Phalen and coworkers (1973) introduced making silicone casts of the airways in situ. We have chosen to use air-dried lungs, similar to Wang and Kraman (1988), to produce the casts. There are several manufacturers of polymer and numerous polymers to chose from. The properties of the polymers are just as diverse. Comparisons of the properties of polymers from the various manufacturers are available but not totally accurate. Five polymers of varying properties were used to make tracheobronchial casts.
Fresh cat, dog, horse, pig and ox lungs were procured f rom local abattoirs and f rom the necropsy laboratory. The heart, esophagus, any other mediastinal tissue and fat were separated from the lungs and tracheobronchial tree similar to McKiernan and Kneller (1983). A cannula of the appropriate diameter was ligated in the trachea. A water source was attached to the cannula and the lungs gently inflated to near capacity. After filling, the water source was removed and the water, mucous and blood allowed to f low out of the trachea. This flushing procedure was repeated 6 to 10 times, until most of the blood and secretions were cleared from the lungs and airways. The surface of the lungs was kept moist during the flushing period. After the majority of the water had drained from the organ, the lungs were inflated and dried using compressed laboratory air directed into the trachea. Smaller lungs were suspended from the trachea and larger lungs were placed on their dorsal (posterior) surface on a tray to contain the extravasated fluid. The air flow was gradually increased until the lungs were inflated and remained inflated to near capacity. Flow and inflation were maintained until the lungs were thoroughly dried (Henry and Butler, 1990).
After drying was complete, the lung was suspended in a vertical position. Aided by an appropriate size funnel, a selected polymer was poured into the trachea and allowed to flow into the lung via gravitational forces. Five polymers were used and two or three casts were made of each polymer. 1. Biodur - S/10/S3/S2 mixture [Biodur Products, Dr. Gunther von Hagens, Rathausstrasse 18, Heidelberg, D- 6900 GERMANY]. 2. Dow Corning - Silastic E RTV [Dow Corning Corp., Midland, Ml 48640-0994, USA]. 3. General Electric - RTV 11 [General Electric Co., Silicone Products Div., Waterford, NY 12188, USA]. 4. & 5. Rhone- Poulenc - 2 different Rhodorsil Silicones: 4. Rhodorsil RTV II - # 1556 and 5. Rhodorsil RTV II - # 1547 [Rhone-Poulenc, Inc., Specialty Plastics Division, CN 5266 , Princeton, NJ 08543- 5266, USA]. All
product components were combined and mixed using the manufacturer's recommendations. Hardener/polymer ratios were 1:10, except Biodur which was 1:100 (S3:S10) but the S2 was varied from 0.5:100 to 2:100 in 0.5 increments. Approximate quantity of polymer used was .2 - .5 kg/ 20 kg dog, 1-2 kg for adult pig, horse or ox. In larger specimens before the silicone hardened, a heavy wire was placed into the lumen of the trachea to give support to the silicone cast. The polymer mixes were allowed to harden over night. The next morning, the lung unit was placed in a vat of simmering to slowly boiling water for several hours.
The specimens were checked in four to five hours to determine if most of the lung and airway tissue had been macerated away from the cast material. Once most of the tissue had been loosened or removed, the cast was removed from the hot water and sprayed with a high pressure hose to remove much of the remaining tissue. If tissue was not removed with the high pressure water, the cast was submerged either in hot water again or in a 10% sodium hydroxide solution until the remaining tissue was released. The specimens were rinsed with water and allowed to dry before use.
All five polymers produced representative casts of the airways or portions of the airways. The more viscous polymers flowed into the terminal bronchi (Fig. 1) and occasionally into the alveoli. The less viscous polymers flowed freely into the alveoli, thus filling the entire airway (Fig. 2). S2 ratios of 1.5 - 2:100 (S10/S3 mix) caused the polymer to harden too quickly, only allowing filling of the larger bronchioles, while casts of S2 0.5:100 ratios remained tacky. The Biodur mix (0.5-1.0:100) consistently was the least viscous and entered the distal airways. The Rhodorsil products usually entered the distal airways. About 30% of the time, Silastic E RTV reached the terminal airways. The GE polymer seldom reached the alveoli. Biodur, Silastic E, and Rhodorsil 1556 produced specimens which had the most elasticity. The GE, Silastic E and Rhodorsil 1547 casts maintained the shape of the lung best.
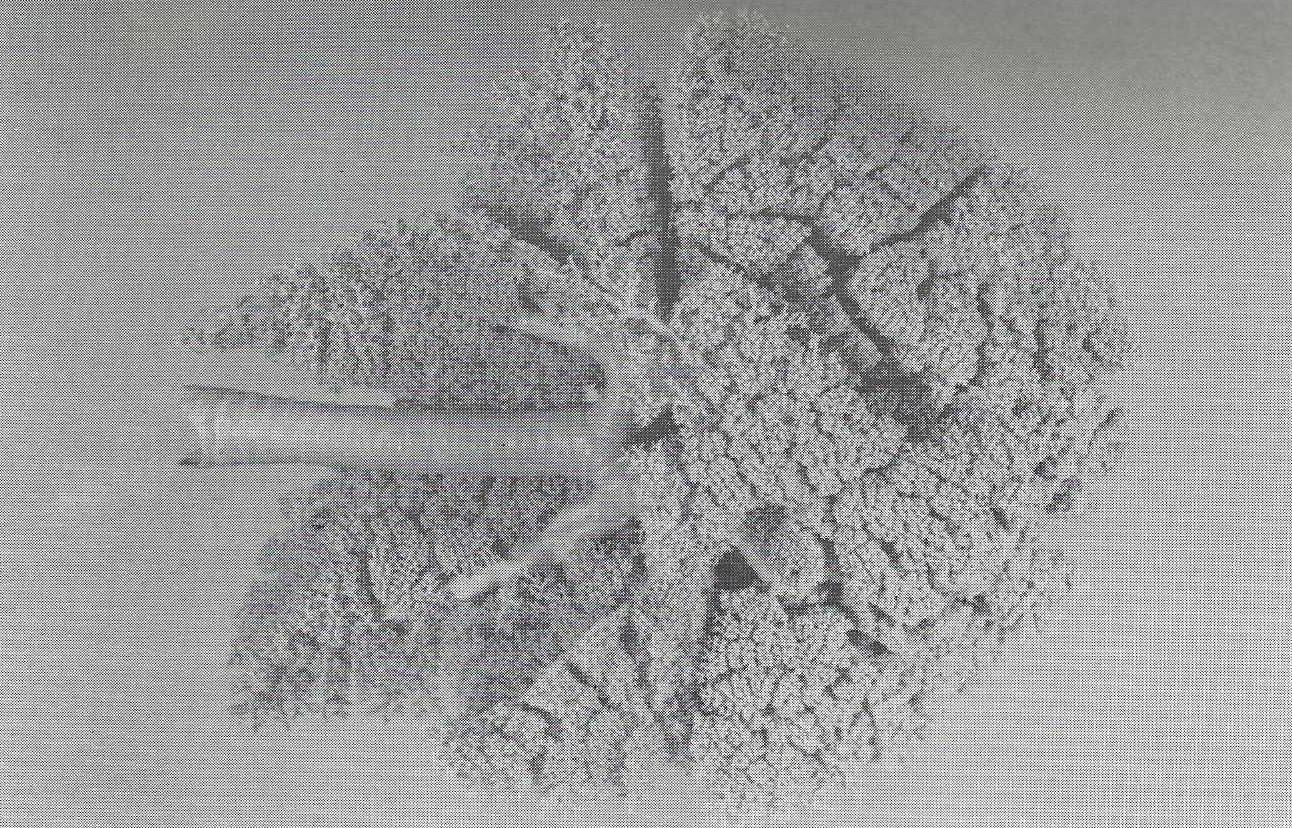 Figure 1. Silicone tracheobronchial cast from a dog. The airways are of # 1547 Rhone-Poulenc polymer mixture (10:1). Note, the airways are filled distally into the alveoli. |
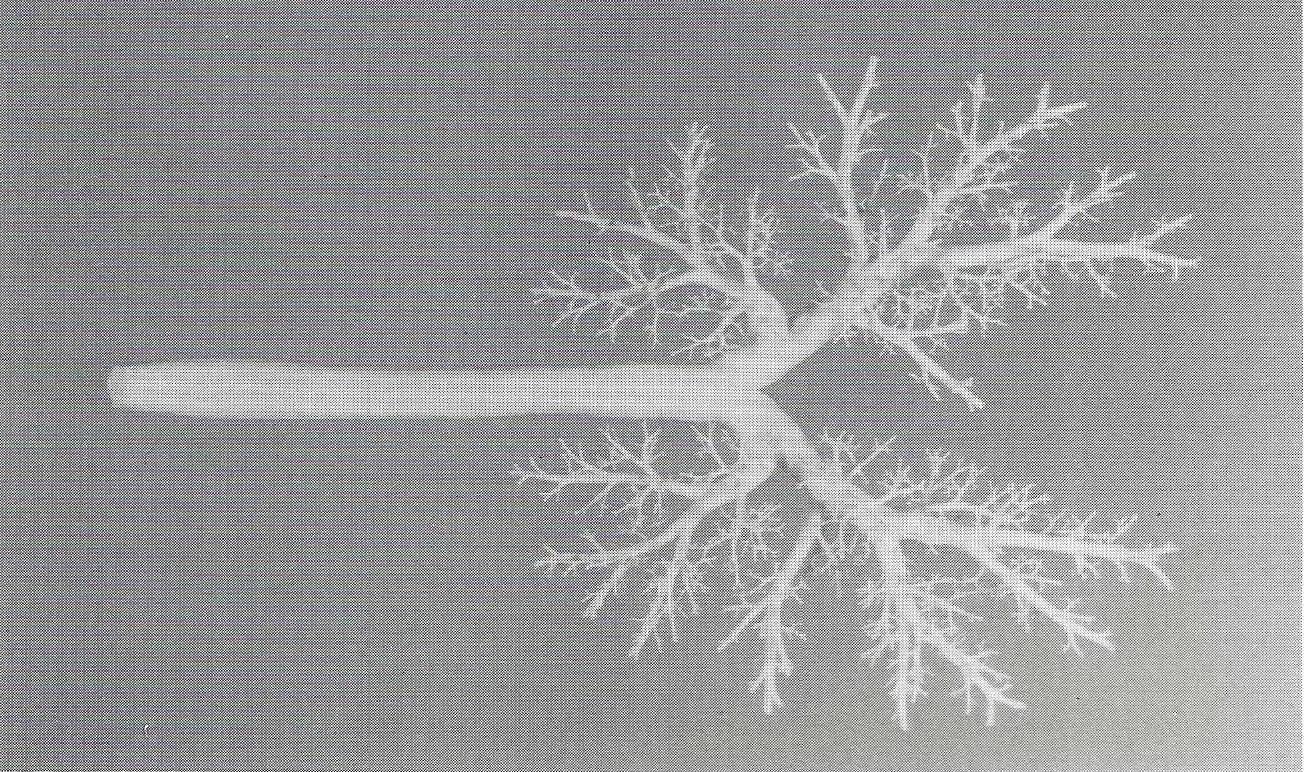 Figure 2. Silicone tracheobronchial from a dog. The airway cast is made of Silastic E RTV polymer mixture (10:1). Note, only the larger airways are filled and the branching pattern is easily observed. |
All six polymers produced durable, representative casts of the airways. The cranial most portion of the cranial (superior) lobes did not fill as uniformly as the caudal (inferior) lobes. This was due to the lungs hanging via the trachea and the least gravitational force was to this area. The type cast which is to be produced must be decided before starting the project. Polymers low in viscosity flow into the alveoli thus filling nearly the entire volume of the lung, whereas more viscous polymers present a more clear view of the branching pattern of the bronchi because less polymer enters the distal airway. Viscosity of the polymer mix may be increased by increasing the time interval between combining the polymer and hardener and actually pouring the mix into the lungs. Therefore, distal airway filling can be decreased or eliminated by waiting 15 minutes to one hour before filling the airway. Thus a cast is produced which allows better visualization of the branching pattern of the airways. All polymer mixes benefited by having a stiff wire inside the tracheal cast for support. The tracheas with the stiff wire insert were better suited to support the airways in a horizontal position, however, steel wire rusted during the maceration process. To prevent rust, a galvanized wire should be used rather than a steel wire. Cost of various polymers is similar, $35.00/kg. Recently, we have used "general household sealant" a 100% silicone rubber product in a caulking tube by General Electric Corporation. The results look promising, especially considering the lower cost, $10.00/kg.
ACKNOWLEDGMENTS
A special thanks to Kreis Weigel and Dr. M. McCracken for help with the photography.
Frank NR, RE Yoder: A method of making a flexible cast of the lung. J Appl Physiol 21:1925-1926, 1966.
https://doi.org/10.1152/jappl.1966.21.6.1925
Henry RW, J Butler: Room-temperature "forced air" impregnation of dried lungs with S10/S3-xylene mix. J Int Soc Plastination 4:14-15,23, 1990.
https://doi.org/10.56507/KTGZ7837
Horsefield K, G Gumming: Morphology of the bronchial tree in man. J Appl Physiol 24:373-383, 1968.
https://doi.org/10.1152/jappl.1968.24.3.373
Kilpper RW, PJ Stidd: A wet-lung technique for obtaining silastic rubber casts of the respiratory airways. Anat Rec 176:279-287, 1973.
https://doi.org/10.1002/ar.1091760304
Mckiernan BC, SK Kneller: A simple method for the preparation of inflated air-dried specimens. Vet Rad 24(2):58-62, 1983.
https://doi.org/10.1111/j.1740-8261.1983.tb01539.x
Tucker Jr. JL, ET Krementz: Anatomical corrosion specimens. Anat Rec 127:655-676, 1957.
https://doi.org/10.1002/ar.1091270404
Phalen RF, HC Yeh, OG Raabe, DJ Velasquez: Casting the lungs in situ. Anat Rec 177:255-263, 1973.
https://doi.org/10.1002/ar.1091770207
Pump KK: Morphology of the acinus of the human lung. Dis Chest 56: 126-134, 1969.
https://doi.org/10.1378/chest.56.2.126
Wang PM, SS Kraman: Construction of a flexible airway model for teaching. Anat Rec 221:780- 781, 1988.
https://doi.org/10.1002/ar.1092210314
Weibel ER, DM Gomez: Architecture of the human lung. Science 137:577-585, 1962.
https://doi.org/10.1126/science.137.3530.577