Department of Pathology Mercer University School of Medicine 1550 College Street Macon, Georgia 31207 USA
During presentation of our (silicone rubber) plastinated gross specimens at national meetings, we have often been questioned about the fate of the specimens' histology. Concern, some of which stems from today's medicolegal climate, has been expressed that the plastination process might destroy or at least alter a specimen's microscopic detail and thus its diagnostic value. Although we had read that plastinated tissue was still suitable for histologic study (1), we elected to undertake the following study with our own specimens.
Silicone;S10;Biodur; Paraffin
AN Walker Department of Pathology Mercer University School of Medicine 1550 College Street Macon, Georgia 31207 USA

![]()



During presentation of our (silicone rubber) plastinated gross specimens at national meetings, we have often been questioned about the fate of the specimens' histology. Concern, some of which stems from today's medicolegal climate, has been expressed that the plastination process might destroy or at least alter a specimen's microscopic detail and thus its diagnostic value. Although we had read that plastinated tissue was still suitable for histologic study (1), we elected to undertake the following study with our own specimens.
Representative blocks were taken from 14 silicone rubber impregnated specimens (eight carcinomas and 6 benign lesions). The sections were immersed in 5% sodium methoxide in methanol for 48 hours to depolymerize the silicone. They were subsequently washed in fresh methanol, processed on an automated tissue processor, embedded in paraffin, and sectioned. Hematoxylin and eosin (H&E) stained slides were prepared simultaneously with routinely processed companion sections of each specimen for comparison.
In each instance, the histologic and cytologic qualities were equal to that of its nonplastinated counterpart. The microscopic appearances were not always identical but diagnostic pathologic features were readily discernable in the deplastinated tissue. In some cases the microscopic appearance of the deplastinated material was judged superior to that of the nonplastinated; this may have been due to better initial fixation of the former. Figure 1 is a high power photomicrograph of a deplastinated, H&E stained section of an esophageal squamous carcinoma. Figure 2 is its nonplastinated counterpart. In both preparations it is possible to see the pleomorphic neoplastic cells, their high nuclear/cytoplasmic ratios, prominent nucleoli and intercellular bridges. The nuclear detail, however, is better preserved in the deplastinated section.
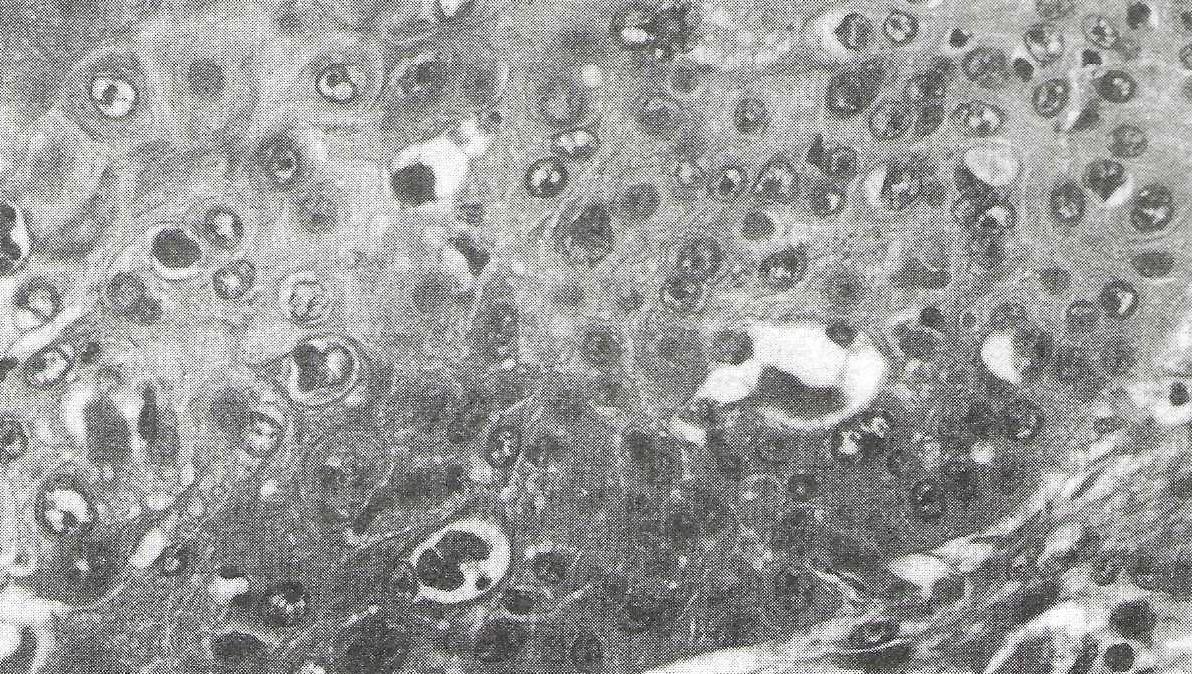 Figure 1: Deplastinated section of a squamous carcinoma of the esophagus (hematoxylin and eosin x 400) |
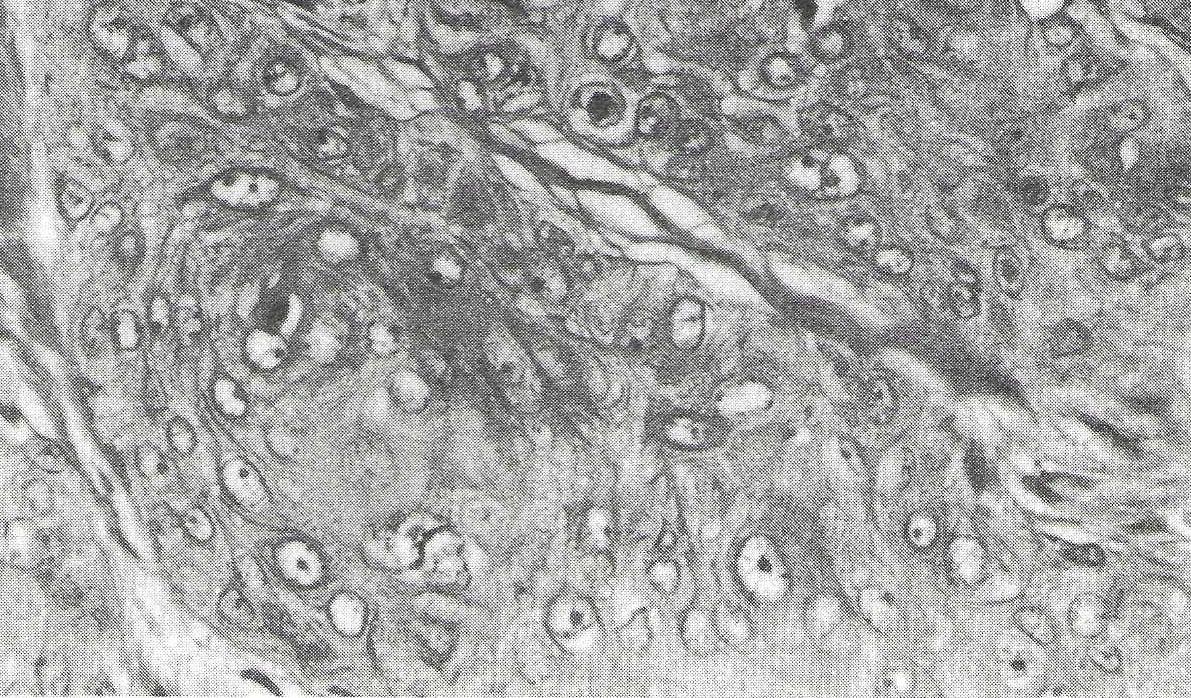 Figure 2: Nonplastinated section of the same tumor, sampled prior to plastination (hematoxylin and eosin x 400) |
One technical aspect to underscore is the absolute necessity of removing all the silicone polymer from the sections prior to processing. Residual silicone will interfere with proper paraffin infiltration and subsequent microscopic slides will be unsatisfactory. We also found initially that deplastinated tissue seemed somewhat resistant to paraffin infiltration and that an enclosed tissue processor with alternating pressure/ vacuum produced better paraffin permeation of the sections.
Under most circumstances there is little call for microscopic examination of plastinated tissue. Our results support those of earlier reports that plastination of a gross specimen does not preclude later histologic study.
1- Klemstein J: Die Histolgie plastinierter (silikonisierter) Organe. MTA Praxis 28:241-248, 1982.