1-Uniformed Services University of the Health Sciences, Bethesda MD;
2-The National Museum of Health & Medicine, Armed Forces Institute of Pathology, Washington, DC;
3-Hartford Hospital, Hartford, CT;
4-UMAB Medical School Anatomical Facility, Maryland Anatomy Board, Baltimore, MD
Human (cadaveric) anatomical preparations have always been an excellent medium for trainees to learn the correct anatomic landmarks and relationships for performing various nerve blocks. The difficulties in handling and the problems of preservation of human anatomical preparations are eliminated with the process of plastination which has received worldwide acceptance for its value in preparing durable material for teaching and museum display.
At The Uniformed Services University of the Health Sciences School of Medicine, The National Naval Medical Center, Bethesda MD., and The Hartford Hospital, Hartford CT, plastinated anatomical sections have been prepared to help establish training aids for teaching regional anesthetic techniques such as brachial plexus block via the interscalene and axillary approaches, subarachnoid, epidural and lumbar plexus blockade, as well as blockade of numerous peripheral nerves of the upper and lower extremity.
Silicone: Body Cross-sections; vascular injection
Pat M. McQuillen, M.D. Uniformed Services University of the Health Sciences, Bethesda MD

![]()



Human (cadaveric) anatomical preparations have always been an excellent medium for trainees to learn the correct anatomic landmarks and relationships for performing various nerve blocks. The difficulties in handling and the problems of preservation of human anatomical preparations are eliminated with the process of plastination which has received worldwide acceptance for its value in preparing durable material for teaching and museum display.
At The Uniformed Services University of the Health Sciences School of Medicine, The National Naval Medical Center, Bethesda MD., and The Hartford Hospital, Hartford CT, plastinated anatomical sections have been prepared to help establish training aids for teaching regional anesthetic techniques such as brachial plexus block via the interscalene and axillary approaches, subarachnoid, epidural and lumbar plexus blockade, as well as blockade of numerous peripheral nerves of the upper and lower extremity.
The plastinated preparations are non-toxic, dry, available for use in any environment, and maintain and reveal precise anatomical detail. In addition, variations in impregnating and curing result in preparations that are resilient and hold up to placement of needles as one would do in performing regional anesthesia. As the needles are advanced through the tissue, a direct visualization of the "the minds eye at the tip of the needle" is appreciated and hand-eye coordination is enhanced.
In these training institutions, the anatomical preparations have received an enthusiastic reception by both instructors and students, with requests and ideas for different regional preparations an applications.
The standard S-10 plastination technique, with its four fundamental steps (fixation, dehydration, forced impregnation and gas curing) was used to prepare human tissue transverse sections which will aid in the teaching of regional anesthetic techniques. Plastination methods described by von Hagens (1985 ) was used as a general guide. Two cadavers relatively young in age, of average body stature, with no apparent trauma and no metastatic processes were selected for the plastination process (Lischka and Prohoda, 1987).
Cadaver 1; The body was kept frozen for several weeks in a deep-freezer, and upon its removal, was sectioned transversely into 1.5 cm sections on a laboratory band saw. To facilitate processing and prevent sections from laying on top of one another, (which impedes the flow of acetone and silicone into the tissue); the sections were layered between aluminum grids lightly fastened with string. The grids were cut to fit into the dehydration and impregnation containers. The strings allowed easy immersion of the whole preparation into the cold acetone and removal from it. A total of twelve sections were fixed by immersion in a 5% formalin solution for several days. After the period of initial fixation, the sections were removed and placed under cold running water to remove excess fixative. This step ensured the removal of any fixative odor and prevented fixative from diluting the dehydration bath later on. The sections were cooled overnight in a refrigerator at +5°c to minimize the chance of ice crystals forming when placed into cold acetone.
Dehydration by freeze-substitution in acetone at - 25°c was used to remove tissue water and some lipids. Dehydration was complete, when the water concentration measured less than 1%. Prior to impregnation, the sections were kept in a bath of warm acetone for one week for additional degreasing. Using Biodur S-1O/S-3 resin, the sections were plastinated by forced impregnation in a vacuum chamber at -25°c, followed by final hardening with the standard gas curing procedure (Baptista et al., 1989; von Hagens, 1985).
Cadaver 2: This body was "lightly" embalmed using a 10% formalin solution. After several days, injection with a mixture of colored (red & blue) S-10 silicone (1%) + S-3 hardener (1%) and S-6 gas cure (2%) via the femoral and axillary vessels was performed. To allow for the silicone to completely harden within the vessels, polymerization time was approximately 48-72 hours. During this time the body was frozen solid and prepared for sectioning. Transverse sections of 1.5 cm were cut on a newly designed band saw. Modifications were made to the standard Hollymatic HiYield 16 meat cutting saw to permit thin frozen slicing of whole body sections with greater precision, and minimal damage, debris and thawing while cutting. The sections were rinsed and cleaned in water and placed directly into cold (-25°c) acetone for dehydration by the freeze-substitution method. With less than one percent residual water in the tissue, the sections were immediately transferred to a vacuum chamber containing a mixture of Biodur S-10/S-3 at -25°c. Vacuum was slowly increased over a four week period, until bubbling ceased on the surface of the silicone. The sections were then removed, drained of excess silicone and cured with S-6 gas cure until the surface was no longer tacky. Additional curing took place in sealed bags for one to two weeks, after which the sections were removed and ready for immediate use.
All of the normal anatomic relations within the sections were maintained following the standard S-10 plastination process. The colorizing material used for injection highlights the vasculature of each section while enhancing its teaching potential. We did, however, observe noticeable blue extravasation in the corpus cavernosum and at other various points where the vessels weakened. This is due most likely to the application of excessive pressure during the injection procedure. These sections, though not aesthetically pleasing like the others, are still useful for teaching. The anatomical positioning of the cadaver should also be considered and appropriately positioned during fixation, otherwise the final product will be distorted (Henry, 1990). The sections from the first cadaver have been shown and demonstrated in a scientific exhibit at the annual meeting of The American Society of Anesthesiologists, and sections produced from the second cadaver will be used to produce an atlas on regional anesthetic techniques.
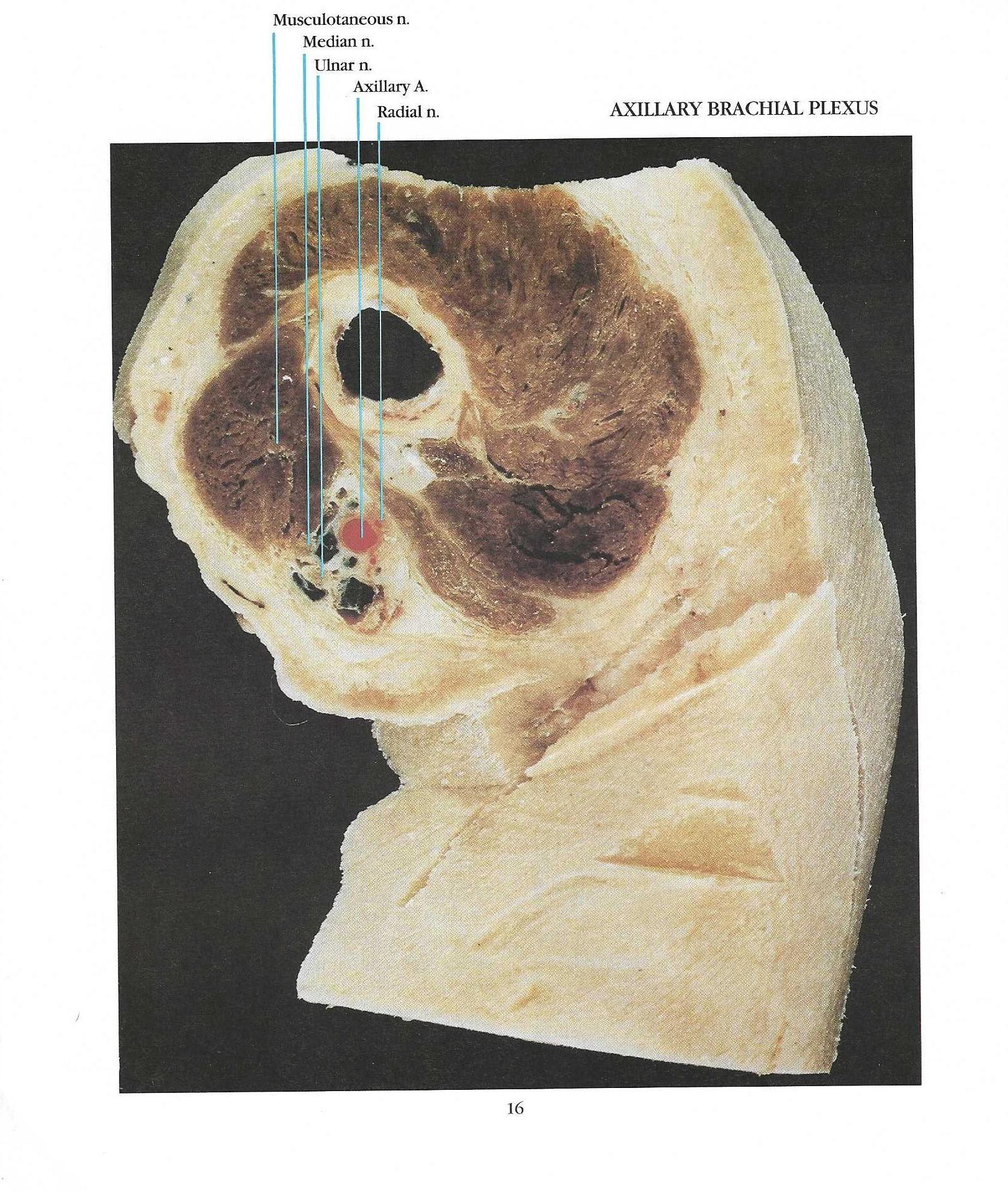 Figure 1. Plastinated cross section of the lumbar subarachnoid space at the level of L4 identifying the subarachnoid space, epidural space, cauda equina, spinous processes and possible approaches to the subarachnoid space with a spinal needle. |
 Figure 2. Specimen of a cross section of the upper arm at the axilla identifying the brachial plexus and the relationship of each of its components to the bone, muscles, vascular structures, and regional block needle. |
Understanding anatomical relationships and correlative anatomy is the cornerstone of a competent practice of regional anesthesia. Plastinated human anatomical preparations for use in teaching regional anesthetic techniques are presently playing a key role in anesthesia education and will have increasing application in the future.
Baptista CAC, M Skie, RA Yeasting, N Ebraheim, WT Jackson: Plastination of the wrist: Potential uses in education and clinical medicine. J Int Soc Plastination 3 (1): 18-21, 1989.
https://doi.org/10.56507/XENF9035
Henry, RW: Preparing and plastinating veterinary anatomy and pathology specimens. Presented at The 5th International Conference on Plastination, Faculty of Medicine, University of Heidelberg, Germany July 1990 J Int Soc Plastination 4 (1): 8, 1990.
Lischka M, M Prohoda: Plastination of whole-body slices with polymerizing emulsion. J Int Soc Plastination 1(1): 17-22, 1987.
https://doi.org/10.56507/TJJM6951
von Hagens, G.: Heidelberg Plastination Folder: Collection of all technical leaflets for plastination. Anatomisches Institut 1, Universitat Heidelberg, 1985.