1Basaveshwara Medical College and Hospital, Chitradurga, Karnataka, India
2J.S.S. Medical College, Mysore, Karnataka, India
The vascular architecture of the suprarenal gland in man varies significantly, which has implications for radiological and surgical procedures. It is important to understand the aberrant suprarenal artery in order to avoid technical hitches during diagnostic and surgical interventions. Fifty specimens, including 34 embalmed human cadavers and 16 fresh specimens from post-mortem bodies, were obtained from the Departments of Anatomy and Forensic Medicine, respectively. Suprarenal arteries were perfused and injected with resin, then painted, and observed for variations in the origin, ramification pattern, and distribution, of the suprarenal arteries. Observations revealed the following variations instead of the usual pattern: 8.33% of right superior suprarenal arteries were branches from the renal artery; the middle suprarenal artery arose from the inferior phrenic artery (20.83% on the right, 19.23% on the left), also, the middle artery was absent: (20.83% on the right 11.54% on the left). The inferior suprarenal artery originated from the aorta (4.16% on the right, 11.53% on the left). Accessary inferior suprarenal arteries arose from superior polar arteries (in 6 specimens on the right and 4 specimens on the left), and from an inferior polar artery (in 4 specimens on the right and 2 on the left side). The outcomes of the present study advocate that in-depth awareness of unusual blood supply of the suprarenal gland is essential for radiological and surgical procedures on retroperitoneal structures of the upper abdomen, to prevent complications.
suprarenal artery; anatomical variations; inferior phrenic artery; aorta; renal artery
Dr. Jyothi Ashok Kumar. Ph.D., Assistant Professor, Department of Anatomy, Basaveshwara Medical College and Hospital,
Chitradurga, Karnataka, India -577502. Tel. +918885333052; Email: jyothiashok.anatomist@gmail.com

![]()



A good knowledge of anatomical variations in the arteries of the abdomen is essential for diagnostic, medical, and surgical practice. The suprarenal gland contains no hilum; hence it is important clinically that the source of the blood supply and the branching pattern of arteries supplying the suprarenal glands are not constant; hence, it is necessary for this to be studied in detail. For instance, a misinterpretation during an angiography procedure, due to the existence of anatomical variants might cause a difficulty in the procedure, and thus a risk of hemorrhage that could be avoided with a sound knowledge of anatomical variations of important blood vessels and their exact ramifications. Anatomical variations of blood vessels are also interesting from a scientific point of view, particularly because of their focus on unresolved issues of ontogeny and phylogeny.
In the mechanism of the stress response, the suprarenal gland plays an important role. The adrenal glands are richly supplied with blood, receiving approximately 5 ml/min (Vinson et al., 1985). Usually, each gland is supplied by three end arteries: the inferior, superior, and middle suprarenal arteries (Merklin, 1962). The arterial network of the suprarenal gland shows species-specific variation. In cats and rats, the arterial plexus is subcapsular and centripetally supplied (Vinson et al., 1985; Bassett & West, 1997), whereas in dogs and humans there exists a capsular arterial plexus, and the cortical and medullary cells are also surrounded by cleft-like sinusoids in the adrenal cortex (Gagnon, 1957; Merklin, 1962; Machado et al., 2001). To minimize complications during surgical interventions on the suprarenal gland, it is critical to have a thorough understanding of both normal and abnormal patterns of the vasculature (Brunt et al., 1996; Sebag et al., 2006). Furthermore, a preoperative vascular investigation is recommended when performing radiological and surgical operations in the subphrenic area, with a focus on the extrahepatic collateral branches (Miękoś 1979; Miyayama et al., 2004; Kim et al., 2005; Dong et al. 2007). The existing literature reveals that the inferior, middle, and superior suprarenal arteries have different origins and branching patterns (Dong et al., 2007; Dutta, 2010). In view of its practical value and embryological basis, the present study aimed to investigate the variations in the origin and branching patterns of both right and left suprarenal arteries.
Fifty specimens were obtained, including 34 embalmed human cadavers from The Department of Anatomy, and 16 fresh specimens from post-mortem bodies (44 males & 6 female specimens, 24 right and 26 left) from the Department of Forensic Medicine, JSS Medical College, MMC, Mysore, and Basaveshwara Medical College and Hospital, Chitradurga, Karnataka, India, from June 2007 to December 2008, and February 2020 to December 2021. Specimens were obtained from cadavers donated with consent for anatomical education and research under the Karnataka Anatomy (Amendment) Act, 1998.
Specimens obtained from the cadaver
In the cadaver, the aorta, inferior phrenic, and renal arteries were identified and cleaned thoroughly, and the suprarenal arteries were traced from their point of origin. Specimens were removed from the cadaver by making a superior and inferior transverse incision at the level of T11 and L3, the former just above the level of the aortic opening of the diaphragm, and the latter at the level of the lower poles of the kidney. The entire retroperitoneal structures were removed en bloc. The aorta was opened by incising the dorsal wall; the openings of the branches were perfused with water and H2O2 to clear clots present in the inferior phrenic, suprarenal, and renal arteries. The specimens were then dried overnight, and the arteries were then washed with acetone to remove water and fat from the branches.
General purpose (GP) resin (Skyline resins, Chennai, India) was mixed with red paint, hardener, and catalyst, in the proportion of 10 ml resin, 2 ml paint, 2 drops hardener, and 2 drops of catalyst. This mixture was injected slowly through the ostia and left overnight for it to settle and harden, which showed the finer branches that we intended to study. The specimens were then preserved in 7% formalin for 20 - 60 days, then dried with a hair drier. A thin solution of Wembley Quickfix adhesive (Wembley House, Gurgaon, India) and acetone (1:10) was coated on to the arteries using a fine brush (00-No), to enable blinding of paint on the vessel wall. Finally, the arteries were painted with PO-red color (Synthetic Enamel Asian paints). Precautions were taken to prevent the addition and mixing up of different arteries. and spilling of paint on to other structures. The paint on the specimen was allowed to dry, then the specimens were numbered and photographed. Specimens were stored immersed in 7% formalin in polythene bags.
Obtaining specimens from post-mortem bodies
An incision was made from the symphysis menti to the symphysis pubis. The thoracic and abdominal cavities were opened, and the organs were removed en bloc. From the en bloc mass, the kidneys, suprarenal glands, and aorta with diaphragm were taken and fixed in standard embalming fluid composed of 10 L 40% formalin, 1 L spirit, 50 g thymol crystal, 500 ml glycerin, 10 L water, 600 g sodium borate, 900 g sodium citrate, 800 g sodium chloride, and 30 ml 1% eosin, for 15 days. Specimens were then prepared as explained above. The origin and branching pattern of the suprarenal arteries were studied from the resulting specimens.
Superior suprarenal artery
In this study, we found 91.66% (22) of right arteries and 100% (26) of left arteries arose from the usual site (i.e., the inferior phrenic artery), whereas on the right side 8.33% (2) of arteries arose from the renal artery. We did not find any superior artery originating from the aorta, superior polar artery, or inferior polar artery, and did not observe the absence of the superior suprarenal artery (Figs. 1, 2, & 5, Tables 1 & 2).
| Origin | RIGHT | LEFT | ||||
| SSR | MSR | ISR | SSR | MSR | ISR | |
| Inferior phrenic artery | 22 | 5 | Nil | 26 | 5 | Nil |
| Aorta | Nil | 8 | 1 | Nil | 18 | 3 |
| Renal artery | 2 | 6 | 23 | Nil | Nil | 23 |
| Superior polar artery | Nil | Nil | 6*1 | Nil | Nil | 4 *1 |
| Inferior polar artery | Nil | Nil | 4*2 | Nil | Nil | 2*2 |
| Absent | Nil | (5) | Nil | Nil | (3) | Nil |
Middle suprarenal artery
We found 33.33% (8) right middle suprarenal arteries originated from the aorta, 20.83% (5) arteries arose from the inferior phrenic artery, 25% (6) arteries arose from the renal artery, and, in 5 specimens (20.83%), did not find the middle suprarenal artery. On other hand, 69.23% (18) left middle suprarenal arteries originated from the aorta, 19.23% (5) arteries from the inferior phrenic artery, and, in 3 (11.54%) specimens, the middle suprarenal artery was absent (Figs. 1, 3, & 5, Tables 1 & 2).
Inferior suprarenal artery
In this study, 95.83% (23) right inferior suprarenal arteries were branches from the usual site, the renal artery. However, 1 right inferior suprarenal artery (4.16%) originated from the aorta. Along with the inferior suprarenal arteries, we observed accessory inferior suprarenal arteries from the superior polar artery in 6 specimens, and from an inferior polar artery in 4 specimens, on the right side. On the left side, 88.46% (23) arteries arose from the renal artery, and 11.53% (3) arteries from the aorta. In 4 specimens, there were accessory inferior suprarenal arteries from the superior polar artery, and two from the inferior polar artery (Figs. 1, 4, & 5, Tables 1 & 2).
|
Artery |
Origin from: |
Absence of artery |
||||
| Inferior phrenic artery | Aorta | Renal artery | Superior polar artery | Inferior suprarenal artery | ||
| Right superior suprarenal artery | 91.66% | 8.33% | 0.00% | 0.00% | 0.00% | 0.00% |
| Left superior suprarenal artery | 100% | 0.00% | 0.00% | 0.00% | 0.00% | 0.00% |
| Right middle suprarenal arteries | 20.83% | 33.33% | 25.00% | 0.00% | 0.00% | 20.83% |
| Left middle suprarenal arteries | 19.23% | 69.23% | 0% | 0.00% | 0.00% | 11.54% |
| Right inferior suprarenal artery | 0.00% | 16.00% | 95.83% | 0.00% | 0.00% | 0.00% |
| Left inferior suprarenal artery | 0.00% | 11.53% | 88.46% | 0.00% | 0.00% | 0.00% |
| Right accessory inferior suprarenal arteries | 0.00% | 0.00% | 0.00% | 25.00% | 16.66% | 0.00% |
| Left accessory inferior suprarenal arteries | 0.00% | 0.00% | 0.00% | 15.38% | 7.69% | 0.00% |
Branches
Branches of the superior suprarenal arteries
The right suprarenal arteries which arose from the inferior phrenic artery gave 2 to 12 branches, whereas arteries that arose from the renal artery gave 6 to 8 branches. On the left side, superior suprarenal arteries that arose from the inferior phrenic artery gave 1 to 11 branches. Interestingly, in one specimen it arose from the right inferior phrenic artery and terminated by giving 4 branches.
Branches of the middle suprarenal arteries
The right middle suprarenal arteries which arose from the aorta gave 2 to 11 branches, while the arteries that arose from the inferior phrenic artery gave 2 to 4 branches, and the arteries which arose from the renal arteries gave 2 to 5 branches. On the other hand, in the case of the left side, the arteries which arose from the aorta gave 0 to 9 branches, the arteries that arose from the inferior phrenic artery also gave 0 to 9 branches, while the arteries from the junction between the renal artery and aorta gave 0 to 3 branches.
Branches of the inferior suprarenal arteries
The right inferior suprarenal arteries from the renal arteries branched into 0 to 12 divisions, whereas the arteries that arose from the aorta gave 0 to 6 branches. The accessory inferior suprarenal arteries which arose from the superior polar artery divided into 2 to 12 branches, and accessory inferior suprarenal arteries from the inferior polar artery divided into 0 to 2 branches. No sex difference was found in variations.
 Figure 1. Graph showing the frequency of the origins of the arteries (SSR: superior suprarenal artery, MSR: middle suprarenal artery, ISR: inferior suprarenal artery, IPA: inferior phrenic artery, RA: renal artery, S Pol: superior polar artery, I Pol: inferior polar artery, ABS: absence) |
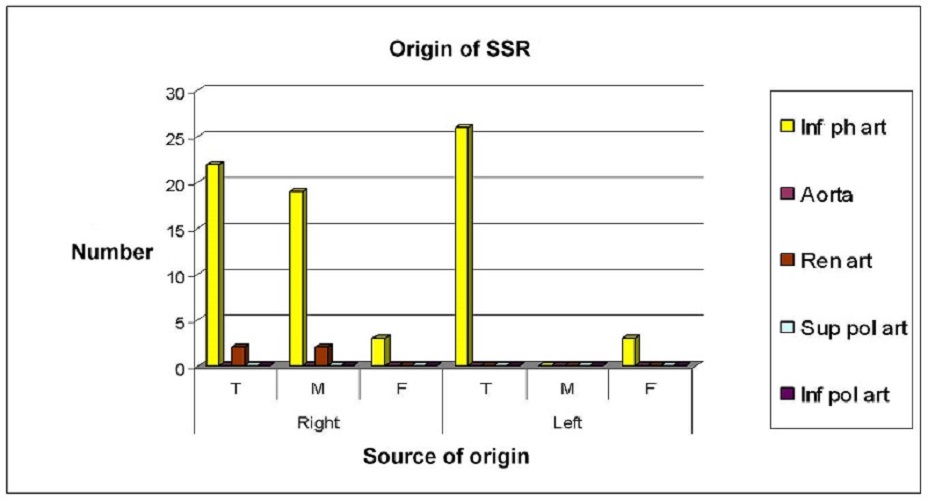 Figure 2. Graph showing the origin of right & left superior suprarenal arteries (Inf ph art: inferior phrenic artery, Ren art: renal artery, Sup pol art: superior polar artery, Inf pol art: inferior polar artery) |
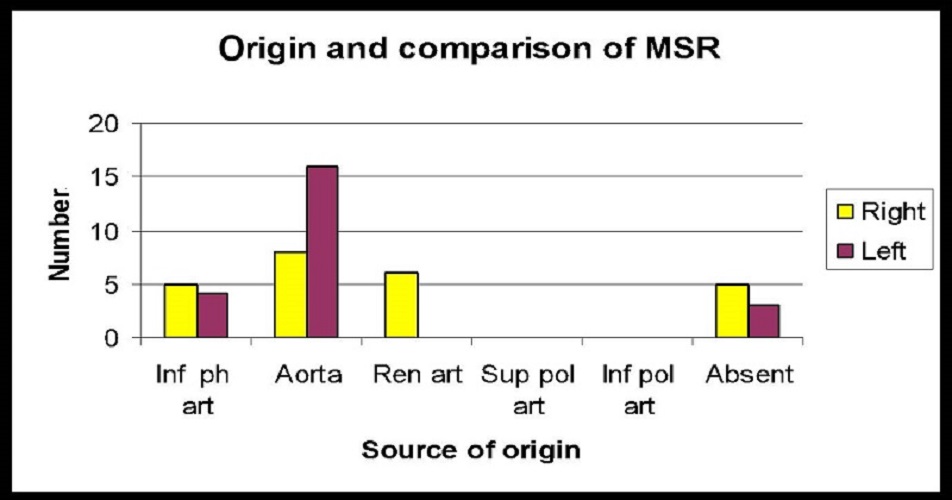 Figure 3. Graph showing the origin of right & left middle suprarenal arteries (Inf ph art: inferior phrenic artery, Ren art: renal artery, Sup pol art: superior polar artery, Inf pol art: inferior polar artery) |
 Figure 4. Graph showing the origin of right & left inferior suprarenal arteries (Inf ph art: inferior phrenic artery, Ren art: renal artery, Sup pol art: superior polar artery, Inf pol art: inferior polar artery). |
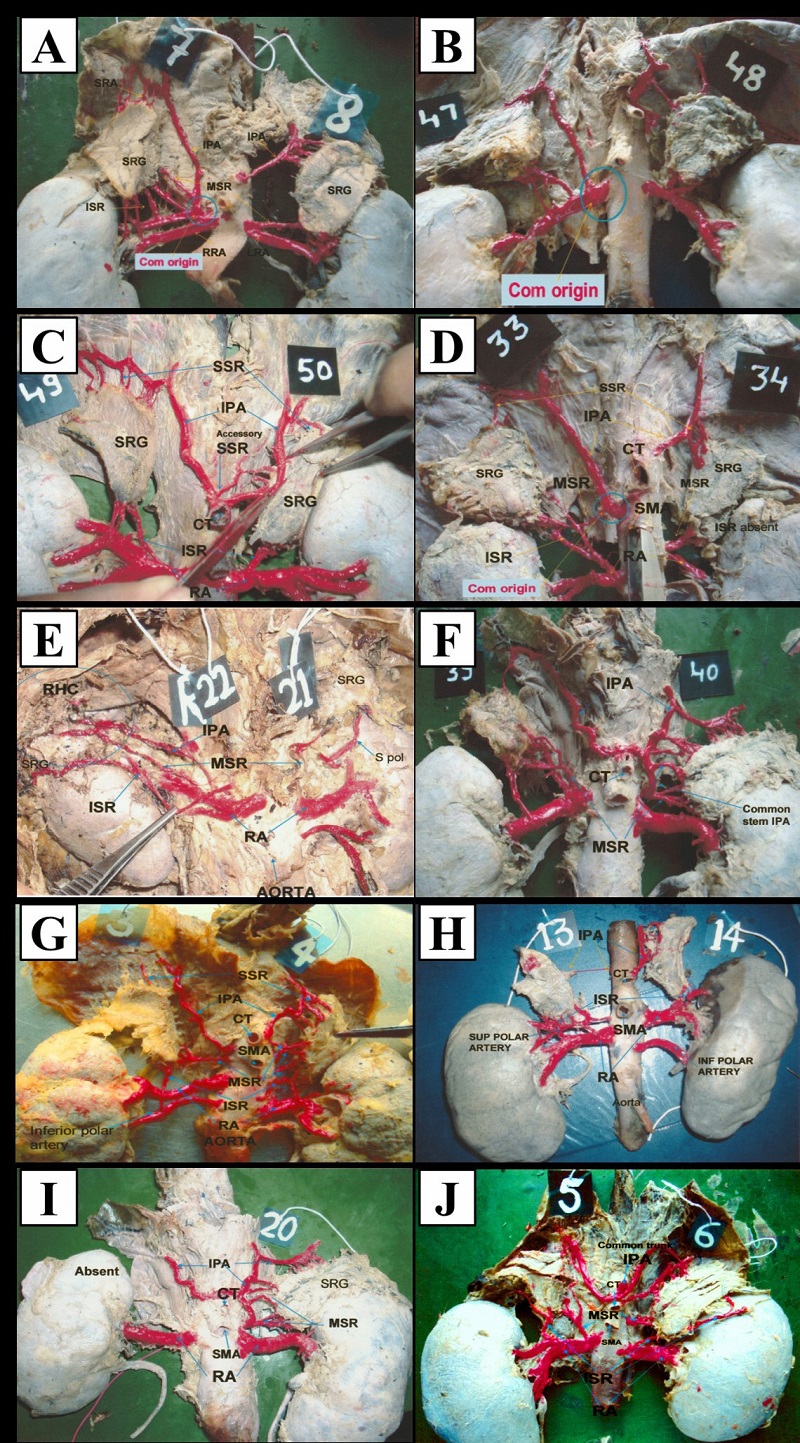 Figure 5. Representative photographs of variations of suprarenal arteries. A & B: all three right suprarenal arteries arose as common trunk from the renal artery; C: left superior suprarenal artery arose from the right inferior phrenic artery; D: very long course of right suprarenal arteries; E: both sides' inferior phrenic arteries arose from the common stem on the left side; F: right accessory inferior suprarenal artery from the inferior polar artery; G: right accessory inferior suprarenal artery from the superior polar artery; H: absence of right suprarenal artery; I: common trunk for both inferior phrenic artery and right middle suprarenal artery arising from the renal artery |
The present study investigated variations in the origin, number, and branching pattern of human suprarenal arteries. Results revealed that variations were present in all three arteries of the suprarenal gland, except for the left superior suprarenal artery. Variations were observed more often on the right side than on the left side, and more in relation to the middle suprarenal artery; the superior suprarenal arteries were next in frequency. During development of the embryo, the lateral splanchnic branches of the dorsal aorta nourish the mesonephros and metanephros kidneys, the gonads, and the suprarenal glands on both sides. Intermediate mesoderm contributes to the development of these structures in part or whole. One gonadal and three suprarenal arteries are normally found on each side of the abdominal aorta. “The definitive superior (inferior phrenic), medial or inferior adrenal arteries originated from the cranial branches of the gonadal artery and/or the abdominal aorta into the adrenocortical blastema. The caudal branches to the gonadal rete blastema reached the metanephros as the definitive renal artery or the preaortic abdominal sympathetic paraganglia. It appears that an accessory renal artery (or arteries) that arose from the aorta above or below the main renal artery originated from an extra branch or branches” (Isogai et al., 2010, p. 668).
Previously, the suprarenal gland was referred to as the suprarenal capsule or adrenal gland, and the blood vessels which supplied this gland were called capsular or adrenal vessels. Based on the Federative Committee on Anatomical Terminology - FCAT (1998) suggestions, the term capsular (1980) and adrenal (in humans) were removed, and blood vessels of the gland were known as suprarenal vessels (FIPAT, 2019). Now the term human adrenal is a misnomer because the human suprarenal gland is present above the kidney (suprarenal), not at the side of the kidney (adrenal) (Gagnon, 1957).
Both in the literature, and in each individual, the number of suprarenal arteries varies. In reality, no two bodies, or even two sides of the same body, have the same blood supply (Merklin & Michels, 1958).
Arteriograms of the inferior suprarenal artery are essential for the diagnosis of tumors of the gland, but the main issue in arteriography of the suprarenal gland is the caliber of arteries, and the large number of arteries and their variations (Rossi, 1968; Rossi et al., 1979). Levi, (1909) demonstrated that the superior suprarenal arteries were numerous, but the middle and inferior suprarenal arteries were solitary (Levi, 1909), but our findings suggested that middle suprarenal artery variations were more frequent than the superior suprarenal artery variations. The earlier reports categorized 7 types of variations in 18 cadavers (Mazza, 1954). The superior suprarenal arteries supply the gland in all circumstances and account for half of the entire number of arteries, while the middle suprarenal arteries provide just 2% of the gland, and the inferior suprarenal arteries account for 30% of the total number of arteries (Gagnon, 1957). On the other hand, Miekos (1979) stated that the inferior suprarenal arteries contributed the largest proportion of blood supply the gland. Diard et al. (1972) described the distribution of the main arteries in the suprarenal gland as follows: the superior suprarenal artery supplies the superior pole and 30 to 50% of the total gland; the middle suprarenal artery supplies the middle portion and 20% of the total gland; and the inferior suprarenal artery supplies the inferior portion and 30 to 50% of the total gland (Dutta, 2010). Lamarque et al. (1973) discovered three vascular pedicles (most commonly two) on radiograms, indicating a bilateral disparity in the blood supply to the suprarenal glands. The superior and inferior pedicles supply the right gland, whereas the superior and intermediate pedicles supply the left gland. According to Toni et al. (1988) the genesis of the suprarenal arteries and their radiological visibility corresponded in the vast majority of instances (Lamarque et al., 1973; Toni et al., 1988). Thus, earlier finding suggested that around 70% of the blood supply to the suprarenal gland is by superior and middle suprarenal arteries, hence, it is essential to acquire sound knowledge about anatomical variations in the origin of these arteries to avoid accidental damage to those arteries during surgeries.
The results of our study demonstrated that the middle suprarenal artery was absent in 50% and 33.3% of specimens on the right and left side, respectively. The semilunar ganglion, celiac plexus, and adipose capsule of the kidney are all supplied by the middle suprarenal artery (Miękoś, 1979), indicating the necessity for extra caution while performing a suprarenal gland segmentectomy. Merklin and Michels (1958) determined that the aorta is the most common source of the middle suprarenal artery, although it can also come from the initial portion of the inferior phrenic artery, the initial segment of the renal artery, the aortic superior polar artery, or the celiac trunk. The results of the present study demonstrate that variations in the origin, branching, and distribution, in all 3 arteries of the suprarenal gland occur, but more frequently in the middle suprarenal arteries, followed by the superior suprarenal arteries; this correlates with earlier studies. Absence of the middle suprarenal gland was found in 20.83% on the right side, while only 11.54% on the left side. The significance of this variation is of great importance to surgeons during nephrectomy and during harvesting of the kidney from donors for transplantation. During the preoperative angiographic study, a detailed observation about the blood supply and variations is indispensable.
The study results showed that variations in the suprarenal arteries are more frequent on the right side. Middle suprarenal artery variations were found most frequently, followed by the superior suprarenal artery. Males and females have no significant differences. The absence of the middle suprarenal and presence of accessory inferior suprarenal arteries have great clinical significance. Knowledge of these variations has relevance and is of great importance for interventional radiologists, oncosurgeons, and transplantation surgeons, when they approach the region either for diagnostic or therapeutic purposes.
Advantages of the plastination method used in this study
There are no poisonous gases or bad odors, making storage of the preserved samples easier. In the long run, it is less expensive than the traditional formalin technique. Specimens can be kept for up to 40 years (more than that of the conventional method). Because all the structures are fully preserved in their near-natural state, plastination provides more detailed features. The topographical anatomy can be also studied in greater detail with the use of sheet plastination (Hayat et al., 2018).
Limitations of the plastination method used in this study
Although plastination is an effective method for preserving specimens, it does have some limits, much like any other approach. Plastinated specimens are relatively rigid (due to the presence of silicone in the tissue), making it difficult to reflect the specimen and display deeper anatomical details. It is difficult to use plastinated specimens for some procedures like ultrasonography and endoscopy due to inflexibility. Similarly, the tissue becomes so hard after plastination that additional dissection is impossible, hence the last dissection must be done before the plastination. Furthermore, because the procedure is a time-consuming and delicate technology, expert staff are required. Plastination laboratory development also necessitates a significant financial investment, which creates a major barrier to the laboratory's development. If the chemicals employed in the plastination technique are not handled appropriately, they might cause health problems (Hayat et al. 2018).
Acknowledgements
The authors sincerely thank those who donated their bodies to science so that anatomical research could be performed. Results from such research can potentially increase mankind’s overall knowledge that can then improve patient care. Therefore, these donors and their families deserve our highest gratitude.
Bassett JR, West SH. 1997: Vascularization of the adrenal cortex: Its possible involvement in the regulation of steroid hormone release. Microsc Res Tech 36(6): 546-557.
https://doi.org/10.1002/(SICI)1097-0029(19970315)36:6<546::AID-JEMT11>3.0.CO;2-O
Brunt LM, Doherty GM, Norton JA, Soper NJ, Quasebarth MA, Moley JF. 1996: Laparoscopic adrenalectomy compared to open adrenalectomy for benign adrenal neoplasms. J Am Coll Surg 183(1): 1-10.
Gwon DI, Ko GY, Yoon HK, Sung KB, Lee JM, Ryu SJ, Seo MH, Shim JC, Lee GJ, Kim HK. 2007: Inferior phrenic artery: anatomy, variations, pathologic conditions, and interventional management. Radiographics 27(3): 687-705.
https://doi.org/10.1148/rg.273065036
Dutta S. 2010: Suprarenal gland-arterial supply: An embryological basis and applied importance. Rom J Morphol Embryol 51(1): 137-140.
FIPAT. 2019: Terminologia Anatomica. 2nd ed. FIPAT.library.dal.ca. Federative International Programme for Anatomical Terminology
Gagnon R. 1957: The arterial supply of the human adrenal gland. Revue Canadienne de Biologie / éditée par l'Université de Montréal 16(4): 421-433.
Hayat K, Qureshi AS, Rehan S, Rehman T. 2018: Plastination-An innovative preservative technique in anatomy. Trends Anat Physiol 1: 003.
https://doi.org/10.24966/TAP-7752/100003
Isogai S, Horiguchi M, Hitomi J. 2010: The para-aortic ridge plays a key role in the formation of the renal, adrenal and gonadal vascular systems. J Anat 216(6): 656-670.
https://doi.org/10.1111/j.1469-7580.2010.01230.x
Kim HC, Jin WC, Lee W, Hwan JJ, Jae HP. 2005: Recognizing extrahepatic collateral vessels that supply hepatocellular carcinoma to avoid complications of transcatheter arterial chemoembolization. Radiographics 25, SPEC. ISS: S25--S39.
https://doi.org/10.1148/rg.25si055508
Lamarque JL, Jaspart W, Delylle A, Senac JP. 1973: Radioanatomie angiographique des surrénales [Angiographic radio-anatomy of the adrenals]. Ann Radiol 16, 549-563. PMID: 4766537. [In French]
Levi G. 1909: Le variazioni delle arterie surrenali e renali studiate col metodo statistico serial [in Italian]. Archivio Italiano di Anatomia e di Embriologia [Italian Journal of Anatomy and Embryology] 8: 35-71.
Machado GV, Gonçalves PR, Parizzi A, Souza JR, Silva MH. 2001: Blood supply of the adrenal glands of nutria (Myocastor coypus - Rodentia: Mammalia). Arch Vet Sci 6(1).
https://doi.org/10.5380/avs.v6i1.3935
Mazza E. 1954: Ricerche anatomiche sulle arterie surrenali dell'uomo [Anatomical research on human adrenal arteries]. Minerva Chirurgica 9(4): 175-181 [In Italian].
Merklin RJ. 1962: Arterial supply of the suprarenal gland. Anat Rec 144(4): 359-371.
https://doi.org/10.1002/ar.1091440407
Merklin RJ, Michels NA. 1958: The variant renal and suprarenal blood supply with data on the inferior phrenic, ureteral, and gonadal arteries: a statistical analysis based on 185 dissections and review of the literature. J Int Coll Surg 29(1 Part 1): 41-76.
Miękoś E. 1979: Anatomical basis of radiodiagnosis of the adrenal gland. Int Urol Nephrol 11(3):193-200.
https://doi.org/10.1007/BF02081960
Miyayama S, Matsui O, Taki K, Minami T, Ito C, Shinmura R, Takamatsu S, Kobayashi M, Notsumata K, Toya D, Tanaka N. 2004: Transcatheter arterial chemoembolization for hepatocellular carcinoma fed by the reconstructed inferior phrenic artery: Anatomical and technical analysis. J Vasc Intervent Radiol 15(8): 815-823. https://doi.org/10.1097/01.RVI.0000136986.34890.D7
Rossi P. 1968: Arteriography in adrenal tumours. Brit J Radiol 41(482): 81-98. doi: 10.1259/0007-1285-41-482-81.
https://doi.org/10.1259/0007-1285-41-482-81
Rossi P, Passariello R, Simonetti G, Rovighi L, Crecco M. 1979: Arterious and venous system of the adrenal glands: anatomical considerations. Ann Radiol (Paris) 22(4): 372-377.
Sebag F, Calzolari F, Harding J, Sierra M, Palazzo FF, Henry J.F. 2006: Isolated adrenal metastasis: The role of laparoscopic surgery. World J Surg 30(5): 888-892.
https://doi.org/10.1007/s00268-005-0342-0
Toni R, Mosca S, Favero L, Ricci S, Roversi R, Toni G, Vezzadini P. 1988: Clinical anatomy of the suprarenal arteries: a quantitative approach by aortography. Surg Radiol Anat 10, 4, 297-302. https://doi.org/10.1007/BF02107902
Vinson GP, Pudney JA, Whitehouse BJ. 1985: The mammalian adrenal circulation and the relationship between adrenal blood flow and steroidogenesis. J Endocrinol 105(2): 285-294.
https://doi.org/10.1677/joe.0.1050285