1Department of Human Morphology, North-Western State Medical University named after I.I. Mechnikov, Saint Petersburg, Russia
2 First Department and Clinic of surgery for the advanced medical education, Military Medical Academy, Saint Petersburg, Russia
3 Center for Anatomy and Molecular Medicine, Sigmund Freud University, Vienna, Austria
Traditional histological slides do not provide visualization of a metal stent and its relationship with the wall inside a coronary artery. A special technique of epoxy plastination of stented coronary arteries was developed to resolve this problem. The specimens used were 14 human hearts with either Bioss, Tryton, or Axcess stents inserted in the coronary arteries. A portion of the heart wall with a stented artery was dehydrated in cold acetone, and impregnated in a vacuum chamber in a mixture of low-viscosity epoxy resin and hardener at a ratio of 20:1. After impregnation, the specimen was left in the resin-mix until the resin was completely cured (7-10 days). The hardened tissue block was ground on an abrasive blade or sawed with a diamond wire band saw into 2 - 3 mm sections. These sections were enclosed in flat chambers in a mixture of epoxy resin and hardener at a ratio of 10:1. This method proved to be reliable to study the relationship of small parts of a stent with the endothelium, to determine changes in the geometry and morphology of bifurcation lesions of stented coronary arteries, and to visualize atherosclerotic lesions within a vessel. Thin 0.5 to 3 mm epoxy resin sections, with a refractive index of 1.45 to 1.51, provided the best transparency for stented coronary arteries. The use of low viscosity epoxy resin ensured impregnation of the tissue. The required transparency was achieved by modifying the refractive index of the resin, by adding dibutylphthalate or another epoxy resin with a lower refractive index to the original epoxy (up to 15%). This plastination method can be applied to research on stents and coronary arteries, and for studying other metal implants.
epoxy plastination; stent; stented coronary arteries; transparent slices
Dmitry Starchik, Repishheva 9-94, Saint Petersburg, 197375, Russia. Telephone: +78129569765; Fax: +78123031853; E-mail: starchik@mail.ru

![]()



The World Health Organization recognizes cardiovascular diseases as a leading cause of death in the world (World Health Organization, 2018), in particular, atherosclerotic lesions of the coronary artery wall, which ultimately lead to narrowing of the vessel and development of coronary heart disease. Currently, metal stents inserted into restricted coronary arteries is the main method used to sustain expansion of the vessel, and prevent coronary disorders (Hajrutdinov and Arablinskij, 2012). However, visualizing the position of a stent and its components inside the coronary artery is still a challenge. Coronary angiography and fluoroscopy with a contrast medium are commonly used for this purpose, but they rarely allow clear observation of the implanted stent. High resolution experimental fluoroscopy makes it possible to visualize the general shape of the stent, but it is difficult to assess the relation of its components with the cells of the vessel wall and atherosclerotic plaques. The lack of clear morphological techniques for studying the microtopography of implanted coronary stents complicates the search for new methods of treating coronary heart disease. The purpose of this study was to develop a new morphological method for visualizing metal stents inside coronary arteries, using plastination.
Fourteen donated human hearts with severe atherosclerotic lesions of the coronary artery walls were used. Metal stents [Axcess (4 specimens), Tryton (5 specimens) and Bios (5 specimens)] had been installed in the affected areas of the arteries by the method of balloon coronary angioplasty under fluoroscopic control.
The epoxy plastination technique was chosen as the basic methodology for the morphological study of metal stents implanted in the coronary arteries. The choice of this method was based on the fact that topography of the investigated anatomical structures is preserved during the entire plastination process (von Hagens et al., 1987). The classic steps of the E12 technique are: preparing thin slices of the desired specimen, cold dehydration, degreasing, impregnation, and finally, curing (von Hagens, 1986; Weber and Henry, 1993; Sora and Cook, 2007; Starchik, 2015; Latorre et al., 2019). Ultra-thin slice plastination produces slices with a maximum thickness of 1 mm down to 0.3 mm (Sora et al., 2019). The epoxy technique also ensures transparency of the connective tissue, which makes it possible to study small anatomical structures in direct and reflected light under magnification of up to 20 times (Sora et al., 2002; Starchik, 2017; Latorre et al., 2019; Sora et al., 2019). After the resin is cured, the epoxy resin-impregnated block becomes very hard. This provides an additional opportunity to use various methods for mechanical processing of plastinated slides without disrupting the original topography of the anatomical and implanted metal structures (Sora, 2007; Starchik, 2008; Sora et al., 2019).
To study stented coronary arteries, a modified epoxy resin plastination protocol was developed, which included 9 stages:
Stage 1: Sections of the heart wall (epicardium and myocardium) with the stented coronary artery 20-50 sq cm, x 10-30 mm thick, were excised.
Stage 2: This anatomical section was dehydrated in -25° C acetone for 3-4 weeks. Acetone was replaced every 7th day. The water content in the acetone solution was determined using an alcohol meter, or by calculation by density of solution. Dehydration was considered complete when the concentration of water in the intermediate solvent/acetone was less than 2%.
Stage 3: Degreasing of the section was performed in order to remove subepicardial fat, which was abundant. This stage is necessary because fat impairs the transparency of plastinated tissues (von Hagens, 1986; Sora, 2007). For degreasing, the anatomical section was placed in pure acetone or methylene chloride at room temperature for two weeks, with one change after 7 days. As lipids enter the solvent, the clear solvent changes to a yellow color. The absence of yellowing of the solution for one week was considered a criterion for the end of degreasing.
Stage 4: The dehydrated and fat-free section of the heart wall was placed in a container of of YD-128 epoxy resin (conventional and optically transparent) and C-403 hardener mixed at a ratio of 20:1. Before impregnation, the transparency coefficient of the epoxy composition was determined with a refractometer to be 1.45-1.51. The container with the specimen was then placed in the vacuum chamber, and the pressure was gradually reduced using a vacuum pump with a mercury manometer control. At pressures below 300 mm Hg, the solvent began to boil and float to the surface of the resin as bubbles. After 24 hours, the resin had impregnated the anatomical block, changed the color of the tissues, and made them transparent. The end of impregnation was realized when the pressure in the chamber was lower than 5 mm Hg, and rare large bubbles were observed.
Stage 5: When impregnation was completed, the sample was removed from the resin and placed in a polyethylene container of an appropriate size for curing at room temperature. Within 2-3 days, the resin stopped flowing from the tissue block and the block was transferred to a 45° С heating cabinet for two weeks until the resin was completely cured.
Stage 6: The hardened blocks were ground with sandpaper or with a grinder to a thickness from 2-4 mm. Some blocks were sawed transversely to produce sections 0.5-2 mm thick. Cross sections of stented coronary arteries were made only after the epoxy resin was completely cured and the tissue block of the heart wall acquired significant hardness. The use of a conventional band saw with the smallest teeth for cross cuts provided poor results, since small elements of the wire often came off the stent during sawing and destroyed the section. In this regard, a special high-speed diamond coated saw blade (EXAKT Advanced Technologies GmbH) was used for making cross sections. Sawing of the cured anatomical block was carried out under water cooling.
Stage 7: At the stage of re-impregnation, the sections were washed in pure acetone for a few seconds to remove sawing/ grinding dust, then placed in a new mixture of YD-128 epoxy resin and C-403 hardener at a 10:1 ratio. Re-impregnation of thin sections was carried out for 3-5 hours in a vacuum chamber until the pressure reached 5-10 mm Hg, when the air and acetone bubbles had been completely eliminated from the samples.
Stage 8: When impregnation was completed, the sections were removed from the resin and placed in flat plexiglass chambers 2-5 mm deep, which were then filled with a new mixture of epoxy resin and hardener, 10:1 ratio. The use of plexiglass for flat chambers eliminates the need for a glass separator (Starchik and Kucher, 2008). The chamber was covered with plexiglass and kept for about 7 days in a 45° С heating cabinet until the resin was completely cured (Sora, 2004).
Stage 9: Flat chambers were dismantled, the plastinated sections were cut to the required size, and then scanned using an office scanner with a resolution from 300-1200 pixels per inch.
This epoxy plastination technique allowed good visualization of metal stents implanted in coronary arteries. The optimal thickness of a thin section after processing of a tissue block should not exceed the thickness/diameter of the stented coronary arteries, 2-3.5 mm. Examination of the sections with a magnifying glass with transmitted or reflected light, or scanning with a high-resolution scanner, made it possible to visualize the entire length of the stent inside the left artery (Fig. 1). Individual stent brands (Axcess and Bios) and their components could be identified as well as their relationship with the arterial wall. One view of an Axcess stent demonstrated that the proximal portion of the stent not against the wall, and the distal portion was compressed by an atherosclerotic plaque. A Bios stent was compressed both proximally and distally. Small and larger atherosclerotic lesions of coronary arteries were observed, as well as small diameter blood vessels branching from the main artery. Lesions were also seen in the acute angle at points of vascular branching. The coronary artery wall in the location of the atherosclerotic plaques was blurred. Another installation of an Axcess stent was done into the bifurcation of the right coronary artery, with a small atherosclerotic plaque located in the area of vessel bifurcation (Fig. 2). Stents were most often located in the main trunk of the coronary vessels. Attempts to install stents into secondary branches were difficult, and often the vessel could not be expanded. Numerous small branches extending from the main trunk of the right coronary artery were also visualized.
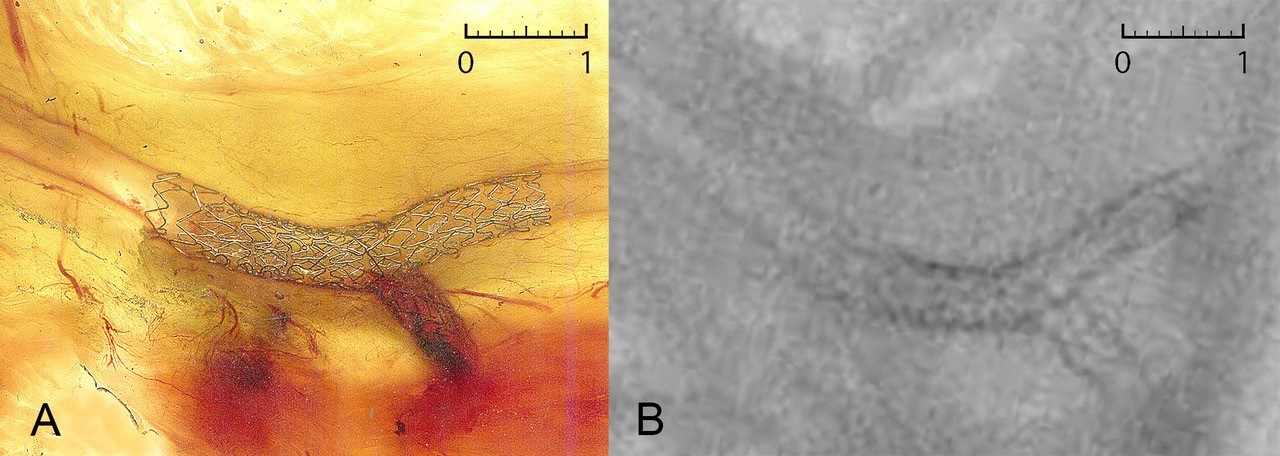 Figure 1: Epoxy plastinated ultrathin section of heart wall. Metal stents in place in left coronary artery - Acess stent does not completely contact the arterial wall proximally (on left) and is compressed distally by plaque. Bios stent (on right) is bounded by atherosclerotic plaque (white) which compresses the stent proximally and distally. Scanning 1200 ppi. Scale bar is 1 cm. |
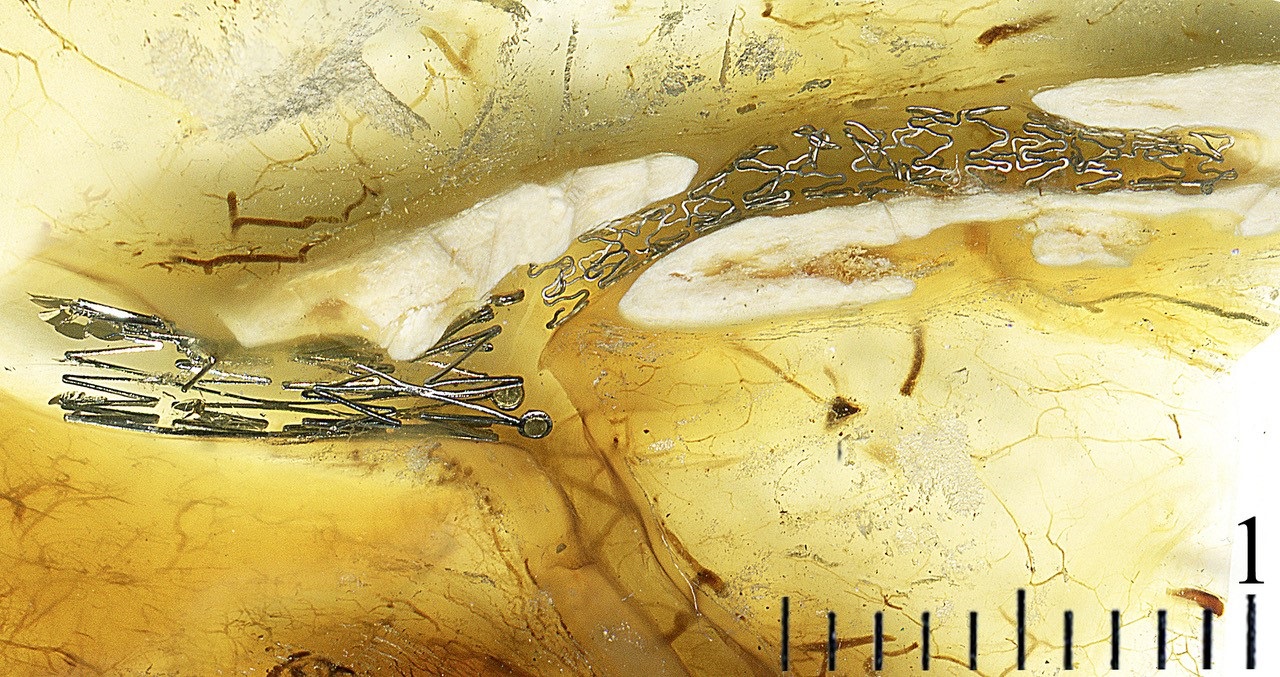 Figure 2: Epoxy plastinated ultrathin section of heart wall. Metal Axcess stent in place in right coronary artery. 1 - Main trunk; 2. - Main branch; 3. - Secondary branch; 4. - Atherosclerotic plaque. Scanning 600 ppi. Scale bar is 1 cm. |
Figure 3A shows an epoxy section of the heart wall with two Tryton metal stents implanted in the left coronary artery bifurcation. The first stent is located in the main trunk of the artery, and extends into its main lateral branch. The second stent of the same type was installed in the secondary branch through the side opening.
The transverse sections of stented coronary arteries were from 0.5-2 mm thick. However, the best results for visualizing stent elements and examining their relations with the vascular wall were achieved with cuts from 0.5-1 mm thick (Fig. 4). The thinness of the resulting sections made it possible to study the plastinated slides under a biological magnifier with a magnification of up to 20x, and to study the relationship of the stent elements in different sections of the vascular wall in cross section. In transverse section, a portion of an Axcess stent was seen to imprint the vessel wall. It was noted that optimal transparency of tissues for research under magnification in transmitted light can be achieved by using an epoxy composition for impregnation with a refraction index from 1.45-1.51.
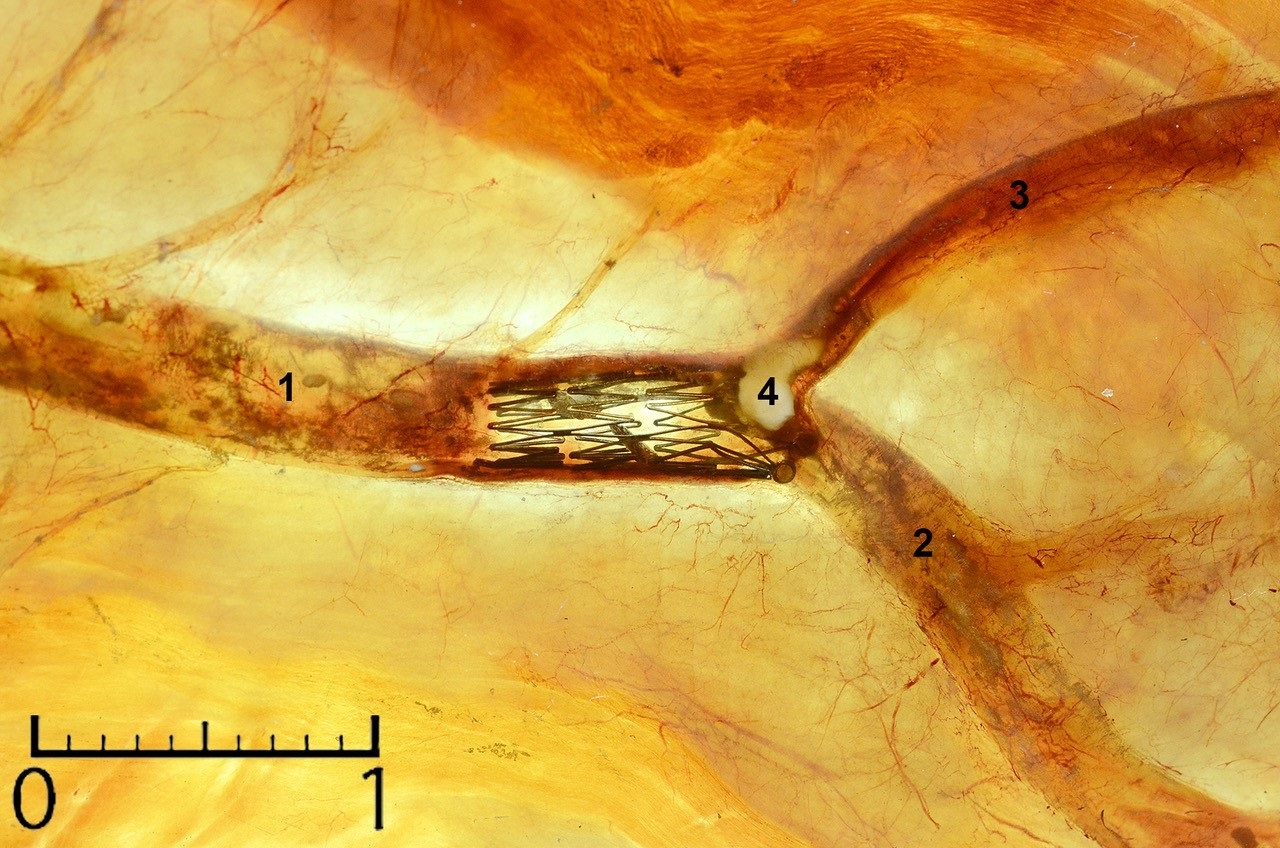 Figure 3: A. Epoxy plastinated ultrathin section, and B. Radiograph of heart wall. Tryton stent in coronary artery and a short Tryton stent into a secondary branch is not patent. Scanning 600 ppi. Scale bar is 1 cm. |
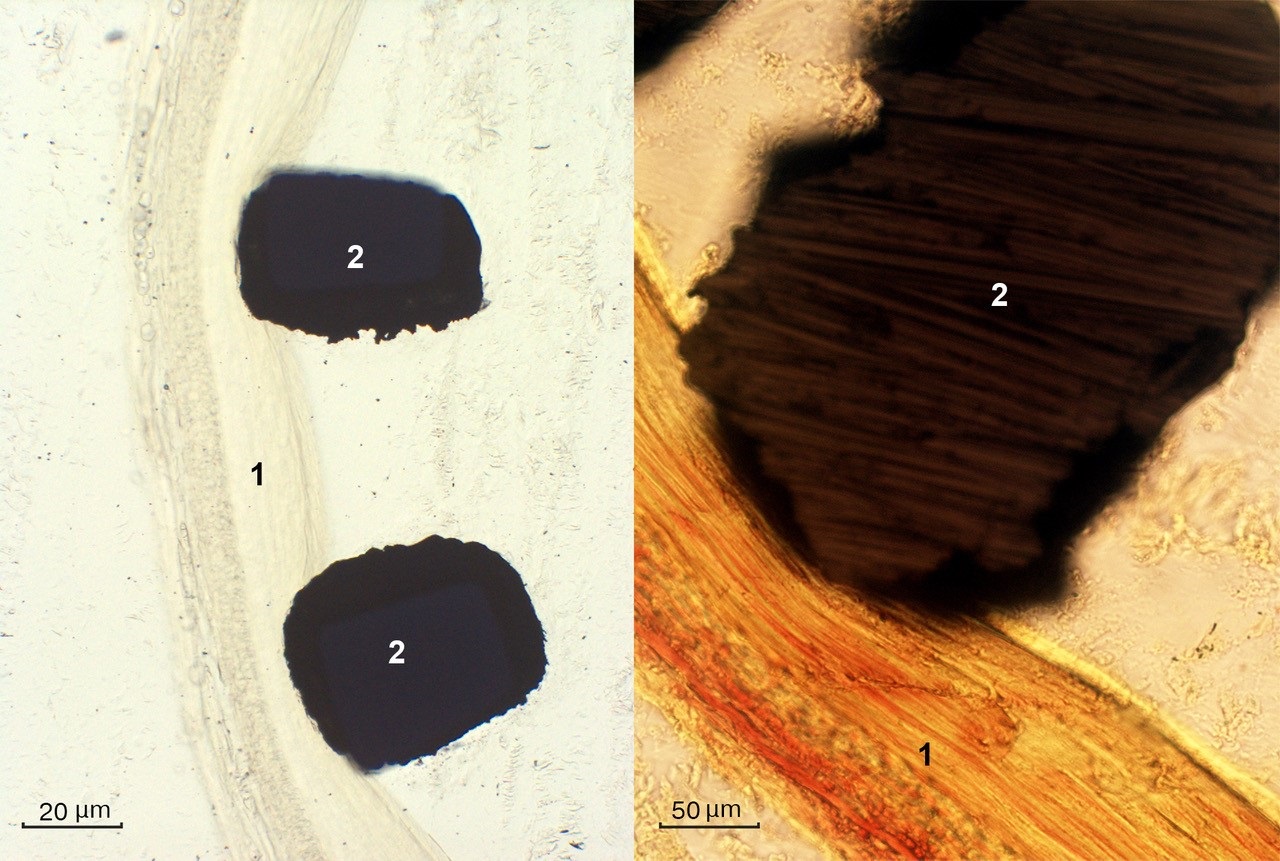 Figure 4: Epoxy plastinated ultrathin transverse section. Bios stent in coronary artery. The inner wall (1) is deformed by the metal stent wire (2). |
Research and clinical studies of stented coronary arteries is limited, as traditional histological methods cannot produce sections thin enough on the microtome due to the metal structure inside the vessel. The epoxy plastination technique reported here makes a solid anatomical block, which firmly secures the tissue and implant within hardened resin. The resulting very hard and durable epoxy block made it possible not only to grind the anatomical block, but also to cut thin sections from it on a diamond blade band saw.
For plastination using this technique, not only formalin-fixed sections can be used, but also biological tissues not preserved at all. It is consistent with the results of other authors using the E12 technique (von Hagens, 1986; Sora and Cook, 2007; Latorre et al., 2019). The plastinated epoxy slices obtained were of high quality (Fig. 1). The transparency and color of the slices were perfect, and shrinkage was not evident. The final epoxy-embedded slices were semitransparent, easy to orientate, and offered much anatomical detail down to the submacroscopic level. The transparent loose areolar and adipose tissues contrasted perfectly with the muscular tissue. The areas of coronary artery bifurcation affected by atherosclerosis are particularly difficult for surgical treatment of a coronary heart disease. The coronary artery wall in the location of the atherosclerotic plaques was often blurred due to the reduced transparency of the tissues.
Axcess stents were often installed in the main trunks of the coronary vessels. Attempts to install this type of stent into secondary branches were difficult, and often the vessel could not be expanded (Fig. 2). Tryton metal stents are usually used for placing in arterial bifurcation areas. This type of stent has small windows which can be used to install another stent in the secondary branch (Fig. 3A, B). Plastinated slides of the heart wall give a more complete morphological picture of the location of a stent inside the coronary artery in comparison to a traditional X-ray. It is clearly visible that, compared to the radiography data (which is traditionally applied in a clinic), the features of the relations between the stents, and the details of their localization in the main trunk of the artery and its branches are visualized much better on the epoxy plastinate.
The proposed technique gives the opportunity to identify the location of atherosclerotic plaques in a vessel and their relations with different parts of a stent, as well as to study the features of coronary artery bifurcation implantation with stents of different designs. This is of interest for improving existing types of stents, and developing new intravascular structures. Plastic coronary stents are not suitable for this technique, since dehydration and degreasing in strong solvents causes deformation of these intravascular implants. Plastinated cross sections of stented coronary arteries ranging from 0.5-1 mm enables study of these slices under magnifications of up to 20x, and also facilitates measurement of the degree of contact of stent elements with the inner tunic of the arterial wall and atherosclerotic plaques.
The best results were achieved using optically transparent YD-128 epoxy resin with a refractive index from 1.45-1.51. Dehydrated and fat-free loose connective tissue, which surrounds the large branches of the coronary arteries, has a similar refractive index. If an epoxy resin is optically transparent and has a similar refractive index, the fabricated plastinated slices become transparent and suitable for investigation in both transmitted and reflected light. Obtaining the desired refractive index was achieved by preliminary measurement of the refractive index of the impregnation epoxy composition with a laboratory refractometer. If the refractive index of a commonly used epoxy is higher than needed, it is possible to modify the refractive index, by adding dibutylphthalate, or another epoxy resin with a lower refractive index, to the original epoxy (up to 15%).
The epoxy plastination sequence described here is more time-consuming than the standard E12 technique, as it includes two stages of impregnation, and also requires certain skills in micro grinding and sawing of cured anatomical blocks. However, the proposed epoxy plastination technique is one of the few methods that allows study of the microtopography of implanted metal stents in coronary arteries without destroying the integrity of the tissues. There is no doubt that, by using this method, it will be possible to investigate other medical devices and structures that can be implanted into the human body, which will significantly expand the possibilities of clinical studies of such devices.
Hajrutdinov ER, Arablinskij AV. 2012: Sovremennye podhody k lecheniyu pacientov s mnogososudistym porazheniem koronarnogo rusla (obzor literatury) [Modern approaches to the treatment of patients with multivessel coronary artery disease (literature review)]. Mezhdunarodnyj zhurnal intervencionnoj kardioangiologii [Int J Interventional Cardioangiology] 29:71-80.
Latorre R, de Jong K, Sora MC, López-Albors O, Baptista C. 2019: E12 technique: Conventional epoxy resin sheet plastination. Anat Histol Embryol 48(6):557-563.
https://doi.org/10.1111/ahe.12507
Sora MC, Strobl B, Staykov D, Traxler H. 2002: Optic nerve compression analyzed by using plastination. Surg Radiol Anat 24:205-208.
https://doi.org/10.1007/s00276-002-0037-2
Sora MC. 2004: High temperature E 12 plastination to produce ultrathin sheets. J Int Soc Plastination, 19:22-25.
https://doi.org/10.56507/NOQQ3899
Sora MC, Cook P. 2007: Epoxy plastination of biological tissue: E12 Technique. J Int Soc Plastination 22:31-39.
https://doi.org/10.56507/FCTY3173
Sora MC. 2007: Epoxy Plastination of Biological Tissue: E12 Ultra-thin Technique. J Int Soc Plastination, 22:40-45.
https://doi.org/10.56507/TQMH6049
Sora MC, von Horst C, López-Albors O, Latorre R. 2019: Ultra-thin sectioning and grinding of epoxy plastinated tissue. Anat Histol Embryol 48(6):564-571.
https://doi.org/10.1111/ahe.12478
Starchik D, Kucher F. 2008: Sheet plastination of whole anatomical objects preserving the natural shape. Abstract presented at The 14th International Conference on Plastination -Heidelberg and Guben, Germany, July 20-26, 2008. J Int Soc Plastination 23:46-47.
Starchik D. 2015: Metodologicheskie osnovy plastinacii raspilov chelovecheskogo tela [Methodological basis for the plastination of body sawcuts]. Morphologia [Morphology] 4:56-61.
Starchik D. 2017: Morfologicheskie i konstitucional'nye osobennosti serdca s uchetom antropometricheskogo statusa i fizicheskogo razvitiya zhenshchin zrelogo i pozhilogo vozrasta [Morphological and constitutional features of the heart, considering the anthropometric status and physical development of mature and old age women]. Avtoref. dis. … d-ra med. nauk [Abstract of dissertation for the degree of Doctor of Medical Sciences]. Moscow: Secenov University, p 36-38.
Von Hagens G, Tiedemann K, Kriz W. 1987: The current potential of plastination. Anat Embryol 175 (4): 411-421.
https://doi.org/10.1007/BF00309677
Von Hagens G. 1986: Heidelberg Plastination Folder: Collection of technical leaflets for plastination. Heidelberg: Anatomiches Institut 1, Universität Heidelberg, p 1-12.
Weber W, Henry RW. 1993: Sheet plastination of body slices - E12 technique, filling method. J Int Soc Plastination, 7(1):16-22.
https://doi.org/10.56507/EZGX2343
World Health Organization. 2018: Global Health Estimates 2016: Deaths by Cause, Age, Sex, by Country and by Region, 2000-2016, Geneva.